
Sleep apnea glossary
Let yourself be surprised by data on correlations that are so far only known to a few specialists, such as sleep apnea and faster aging or sleep apnea and negative changes in the intestinal flora.
Please write to us if you are missing certain answers or information, would like to contribute new knowledge or research results, or have a question about the content.
The glossary is arranged alphabetically, including the sub-items of individual main topics.
AHI
The severity of sleep apnea syndrome is indicated by the apnea-hypopnea index (AHI). This indicates the number of apneas and hypopneas per hour. (1)
Apnea-hypopnea index (AHI) – classification and definition: mild = 5 – 14 respiratory arrests per hour moderate = 15 – 29 respiratory arrests per hour severe = > 30 respiratory arrests per hour
Note: The fact that the "hard" category starts at 30 does not mean that 35 or 40 are already very high values. AHI scores of 50 or 60 are not uncommon. In one study, a value of 107 (!!) is reported. (2)
Sources
(1) Apnea-hypopnea index – https://de.wikipedia.org/wiki/Apnoe-Hypopnoe-Index
(2) Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995 Oct; 96(4):1897-904. doi: 10.1172/JCI118235. PMID: 7560081; PMCID: PMC185826. – https://pmc.ncbi.nlm.nih.gov/articles/PMC185826/
Apneas and hypopneas
Apnea (from ancient Greek "non-breathing") is a complete closure of the respiratory tract. This means a complete interruption of inhalation, a drop in oxygen saturation in the blood and, as a result, negative changes in metabolism.
Hypopnea is a partial obstruction of the respiratory tract. By definition, hypopnea is a reduction in breathing depth by at least 50% over a period of at least 10 seconds. This is also enough for a significantly reduced oxygen supply. Hypopneas are less severe than apneas, but can be the precursor to apneas or occur alternately with them.
TMD (craniomandibular dysfunction)
TMD is a functional disorder that mainly affects the jaw and temporomandibular joints, but which also involves the masticatory muscles and teeth. However, this orthopaedic problem, which at first glance seems simple, has far-reaching consequences. Diagnosis is difficult, which also affects the right treatment. It is particularly treacherous that the symptoms triggered by TMD can occur both in the head and in completely different parts of the body.
Typical consequences in the head area are teeth grinding, tooth neck defects, uneven/restricted mouth opening, jaw pain, joint cracking, visual disturbances, dizziness, ringing in the ears, difficulty swallowing and headaches/migraines. The body can experience neck, shoulder, back and joint pain, including herniated discs, numbness of the arms and fingers as well as reduced performance.
The Society for Dental Health, Function and Aesthetics (GZFA) suspects that about 20 percent of the population have jaw symptoms in need of treatment. A good third grind and clench their teeth at night, which can lead to the aforementioned functional disorders. The primary cause is considered to be stress, which is "processed" by grinding.
A very successful solution is a grinding, repositioning bzw. CMD splint. This has led to exciting results in studies. In Garner's study (1), researchers were able to measure better gas exchange, less lactate and less cortisol during exercise. Which, conversely, means less stress and more relaxation. In a second study, he found a reduced breathing volume at the same intensity of exertion. (2) Researchers found improved breathing economy in basketball players (3) and an increase in performance in swimmers. Martins et. al. demonstrated an increase in performance during aerobic and anaerobic exercise. (4)
The results show how strongly this rather inconspicuous functional disorder affects breathing and metabolic parameters. And of course, this can be transferred to the stress of the non-athlete.
Sources
(1) Garner DP, Dudgeon WD, Scheett TP, McDivitt EJ. The effects of mouthpiece use on gas exchange parameters during steady-state exercise in college-aged men and women. J Am Dent Assoc. 2011 Sep; 142(9):1041-7. doi: 10.14219/jada.archive.2011.0325. Erratum in: J Am Dent Assoc. 2012 Mar; 143(3):228 – https://pubmed.ncbi.nlm.nih.gov/21881071/
(2) Garner DP. Effects of various mouthpieces on respiratory physiology during steady-state exercise in college-aged subjects. Gen Dent. 2015 Nov-Dec; 63(6):30-4. Erratum in: Gen Dent. 2016 Jan-Feb; 64(1):79 – https://pubmed.ncbi.nlm.nih.gov/26545272/
(3) Schulze A, Kwast S, Busse M. Effects of a Vented Mouthguard on Performance and Ventilation in a Basketball Field Setting. J Sports Sci Med. 2019 Jun 1; 18(2):384-385. – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6543990/
(4) Miró A, Buscà B, Solana-Tramunt M, Aguilera-Castells J, Arboix-Alió J, Vergnoux F, Arellano R. Effects of wearing a customized bite-aligning mouthguard on powerful actions in highly trained swimmers. J Exerc Sci Fit. 2021 Oct; 19(4):259-268. doi: 10.1016/j.jesf.2021.09.003. Epub 2021 Oct 2 – https://pubmed.ncbi.nlm.nih.gov/34712336/
(5) Schultz Martins R, Girouard P, Elliott E, Mekary S. Physiological Responses of a Jaw-Repositioning Custom-Made Mouthguard on Airway and Their Effects on Athletic Performance. J Strength Cond Res. 2020 Feb; 34(2):422-429. – https://pubmed.ncbi.nlm.nih.gov/29927893/
CPAP / APAP / PAP
These are the abbreviations for "positive airway pressure" (PAP), "continuous positive airway pressure" (CPAP) and "auto positive airway pressure" (APAP), in german 'positive airway therapy'. Adaptive servo ventilation (ASV) is one of the newer forms of positive airway therapy. Unlike the fixed pressure of a CPAP machine, the pressure in ASV continuously adjusts and triggers breathing according to the patient's breathing patterns when needed. This makes ASV particularly useful for patients with central sleep apnea. (1)
This refers to the method used for sleep apnea, in which air is directed into the airways with a slightly higher pressure than the surrounding air pressure with a device. This keeps the upper airways open. This makes it easier for patients to breathe in and prevents the typical symptom of sleep apnea: the occlusion of the airways. The person concerned receives a full-face or mouth-nose mask. People who breathe through their nose at night can use a nose-only mask, which covers the face less. In the literature, a duration of 4 hours per night is usually considered the minimum for effective use. (2)
Sources
(1) Advantages and disadvantages of adaptive servo ventilation (ASV) for sleep apnea – https://gobend2020.com/de/vor-und-nachteile-der-adaptiven-servo-ventilation-asv-bei-schlafapnoe/
(2) Bosschieter PFN, Uniken Venema JAM, Vonk PE, Ravesloot MJL, Hoekema A, Plooij JM, Lobbezoo F, de Vries N. Equal effect of a noncustom vs a custom mandibular advancement device in treatment of obstructive sleep apnea. J Clin Sleep Med. 2022 Sep 1; 18(9):2155-2165. doi: 10.5664/jcsm.10058. PMID: 35532113; PMCID: PMC9435323. – https://pubmed.ncbi.nlm.nih.gov/35532113/
CPAP / APAP - Devices
CPAP and APAP devices are available separately as standalone devices or as a combination in one device. This is marked accordingly. APAP and CPAP devices are very similar in terms of purchase price. Prices are usually between 700 and 2000 euros, while small appliances for overnight stays away from home are cheaper. If prescribed by the family doctor or sleep specialist, the health insurance company will cover part of the costs. Special equipment for the clinic is much more expensive at 5000 – 6000 euros.
CPAP / APAP - health benefits
Despite PAP, respiratory arrests in the range of 5 to 10 apnea and hypopnea events per hour still remain (residual events). (1) Therapy with CPAP machines is purely symptomatic, there is only a limited prospect of improvement of sleep apnea and at the same time of concomitant diseases. (2) Two studies showed that the use of CPAP did not reduce the incidence of cardiovascular disease and premature death. (3)(4) Another study even came to the conclusion that people with heart failure experienced higher all-cause mortality and cardiovascular mortality during ASV (adaptive servoventilation) treatment. Although the treatment had lowered the AHI score to an average of 6.6. The number of primary endpoints (death or life-threatening development) was the same in the treatment and control groups. The observation of the patients lasted between 2 and 7 years, due to constant recruitment. (5) These results led to dramatic changes in clinical practice, with the frequency of prescribing servo ventilation declining due to changes in guidelines. And also to the fact that exactly this type of device is no longer used. (6) The lack of effect of CPAP in obese patients with apnea supports the view that sleep apnea and drowsiness in obese patients may rather be an expression of overweight and metabolic syndrome. (7)
Sources
(1) O'Connor GT, Caffo B, Newman AB, Quan SF, Rapoport DM, Redline S, Resnick HE, Samet J, Shahar E. Prospective study of sleep-disordered breathing and hypertension: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2009 Jun 15; 179(12):1159-64. doi: 10.1164/rccm.200712-1809OC. Epub 2009 Mar 5. PMID: 19264976; PMCID: PMC2695498. – https://pubmed.ncbi.nlm.nih.gov/19264976/
(2) Dr. Berndsen: Sleep apnea – CPAP and ASV – long-term use with positive or negative effects? – https://www.youtube.com/watch?v=Wzde-LteCJI
(3) Guimarães TM, Poyares D, Oliveira e Silva L, Luz G, Coelho G, Dal Fabbro C, Tufik S, Bittencourt L. The treatment of mild OSA with CPAP or mandibular advancement device and the effect on blood pressure and endothelial function after one year of treatment. J Clin Sleep Med. 2021 Feb 1; 17(2):149-158. doi: 10.5664/jcsm.8822. PMID: 32964829; PMCID: PMC7853217. – https://pubmed.ncbi.nlm.nih.gov/32964829/
(4) Yu J, Zhou Z, McEvoy RD, Anderson CS, Rodgers A, Perkovic V, Neal B. Association of Positive Airway Pressure With Cardiovascular Events and Death in Adults With Sleep Apnea: A Systematic Review and Meta-analysis. JAMA. 2017 Jul 11; 318(2):156-166. – https://pubmed.ncbi.nlm.nih.gov/28697252/
(5) Cowie MR, Woehrle H, Wegscheider K, Angermann C, d'Ortho MP, Erdmann E, Levy P, Simonds AK, Somers VK, Zannad F, Teschler H. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N Engl J Med. 2015 Sep 17; 373(12):1095-105. doi: 10.1056/NEJMoa1506459. Epub 2015 Sep 1. PMID: 26323938; PMCID: PMC4779593. – https://pubmed.ncbi.nlm.nih.gov/26323938/ + https://link.springer.com/article/10.1007/s15005-015-1527-1
(6) Correia S, Sousa S, Drummond M, Pinto P, Staats R, Brito D, Lousada N, Cardoso JS, Moita J. Diagnostic and therapeutic approach of central sleep apnea in heart failure – the role of adaptive servo-ventilation. A statement of the Portuguese society of pulmonology and the Portuguese sleep association. Pulmonology. 2022 Apr 29:S2531-0437(22)00005-8. doi: 10.1016/j.pulmoe.2021.12.002. Epub ahead of print. PMID: 35501278 – https://pubmed.ncbi.nlm.nih.gov/35501278/
(7) Vgontzas AN, Bixler EO, Chrousos GP. Sleep apnea is a manifestation of the metabolic syndrome. Sleep Med Rev. 2005 Jun; 9(3):211-24. doi: 10.1016/j.smrv.2005.01.006. PMID: 15893251. – https://pubmed.ncbi.nlm.nih.gov/15893251/
CPAP / APAP - Measurement Accuracy
A completely different point is the discussion about the poor comparability of the data collected with CPAP compared to polysomnography. A 2022 study describes significant and persistent differences between manually detected and automatically detected apnea events during PAP therapy. To make matters worse, CPAP machine manufacturers use different definitions for what is registered as apnea and hypopnea. (1)(2)(3) Therefore, there has been a trend towards automatic PAP therapy (APAP) and supervised therapy with telemedicine for several years. (3)
Sources
(1) Bertelli F, Suehs CM, Mallet JP, Rotty MC, Pepin JL, Gagnadoux F, Matzner-Lober E, Bourdin A, Molinari N, Jaffuel D. Apnoea-hypopnoea indices determined via continuous positive airway pressure (AHI-CPAPflow) versus those determined by polysomnography (AHI-PSGgold): a protocol for a systematic review and meta-analysis. BMJ Open. 2021 May 10; 11(5):E044499. doi: 10.1136/bmjopen-2020-044499. – https://pubmed.ncbi.nlm.nih.gov/33972338/
(2) Ni YN, Thomas RJ. A longitudinal study of the accuracy of positive airway pressure therapy machine-detected apnea-hypopnea events. J Clin Sleep Med. 2022 Apr 1; 18(4):1121-1134. doi: 10.5664/jcsm.9814. – https://pubmed.ncbi.nlm.nih.gov/34886948/
(3) Dusart C, Andre S, Mettay T, Bruyneel M. Telemonitoring for the Follow-Up of Obstructive Sleep Apnea Patients Treated with CPAP: Accuracy and Impact on Therapy. Sensors (Basel). 2022 Apr 5; 22(7):2782. doi: 10.3390/s22072782. – https://pubmed.ncbi.nlm.nih.gov/35408395/
CPAP / APAP - Disadvantages
Anyone who starts PAP therapy has a more or less long time to get used to the mask and unnatural breathing against resistance. The mask is unfamiliar and uncomfortable. Not everyone can cope with the mask. (1) For each overnight stay away from home, the user must have the entire equipment with him. The CPAP devices can only be individually adjusted to the sleep behavior of the individual user to a limited extent. For the exact adjustment of the devices, a session in the sleep laboratory must be attended, depending on the patient's condition. (2)
There are restrictions – not everyone is allowed to use CPAP machines (e.g. for lung diseases such as COPD, obesity hypoventilation syndrome).
And, there are two major disadvantages of CPAP therapy that are often concealed: a) Patients often experience feelings of pressure and shortness of breath when exhaling against the incoming air flow. b) The use of CPAP decreases very significantly within the first year after the first application of the method. (3) If you don't use CPAP regularly at the beginning, you won't do it later. The drop-out rate is very high, based on figures from a Canadian and Japanese sleep center. (4)(5)(6) Controls showed that the acceptance of CPAP is better in patients with high AHI than in people with low AHI. (7)(8)
Sources
(1) Ferraz PD, Francisco I, Borges MI, Guimarães A, Carvalho F, Caramelo F, Figueiredo JP, Vale F. Pharyngeal Airspace Alterations after Using the Mandibular Advancement Device in the Treatment of Obstructive Sleep Apnea Syndrome. Life (Basel). 2022 Jun 2; 12(6):835. doi: 10.3390/life12060835. PMID: 35743866; PMCID: PMC9224702. – https://pubmed.ncbi.nlm.nih.gov/35743866/
(2) Jaffuel D, Mallet JP, Sabil A. Accuracy of continuous positive airway pressure devices: the devil is in the details, the best is yet to come. Sleep Breath. 2022 Nov 17. doi: 10.1007/s11325-022-02741-9. Epub ahead of print. – https://pubmed.ncbi.nlm.nih.gov/36394693/
(3) Narang I, Kendzerska T, Heffernan A, Malik U, Carvalho CG, Ryan CM. Positive Airway Pressure Usage in Youth with Obstructive Sleep Apnea Following Transition to Adult Health Care. Nat Sci Sleep. 2022 Feb 2;14:153-163. doi: 10.2147/NSS. S345143. PMID: 35140537; PMCID: PMC8818969. – https://pubmed.ncbi.nlm.nih.gov/35140537/
(4) Colvin LJ, Dace GA, Colvin RM, Ojile J, Collop N. Commercial Motor Vehicle Driver Positive Airway Pressure Therapy Adherence in a Sleep Center. J Clin Sleep Med. 2016 Apr 15; 12(4):477-85. doi: 10.5664/jcsm.5670. PMID: 26715403; PMCID: PMC4795273. – https://pubmed.ncbi.nlm.nih.gov/26715403/
(5) Hsu N, Zeidler MR, Ryden AM, Fung CH. Racial disparities in positive airway pressure therapy adherence among veterans with obstructive sleep apnea. J Clin Sleep Med. 2020 Aug 15; 16(8):1249-1254. doi: 10.5664/jcsm.8476. PMID: 32267221; PMCID: PMC7446068. – https://pubmed.ncbi.nlm.nih.gov/32267221/
(6) Patel N, Sam A, Valentin A, Quan SF, Parthasarathy S. Refill rates of accessories for positive airway pressure therapy as a surrogate measure of long-term adherence. J Clin Sleep Med. 2012 Apr 15; 8(2):169-75. doi: 10.5664/jcsm.1772. PMID: 22505862; PMCID: PMC3311414. – https://pubmed.ncbi.nlm.nih.gov/22505862/
(7) Furukawa T, Suzuki M, Ochiai M, Kawashima H, Yokoyama N, Isshiki T. Long-term adherence to nasal continuous positive airway pressure therapy by hypertensive patients with preexisting sleep apnea. J Cardiol. 2014 Apr; 63(4):281-5. doi: 10.1016/j.jjcc.2013.08.013. Epub 2013 Oct 20. PMID: 24148860. – https://pubmed.ncbi.nlm.nih.gov/24148860/
(8) Madbouly EM, Nadeem R, Nida M, Molnar J, Aggarwal S, Loomba R. The role of severity of obstructive sleep apnea measured by apnea-hypopnea index in predicting compliance with pressure therapy, a meta-analysis. On the J Ther. 2014 Jul-Aug; 21(4):260-4. doi: 10.1097/MJT.0b013e318249a09d. PMID: 22407199 – https://pubmed.ncbi.nlm.nih.gov/22407199/
CPAP / APAP - Side effects of the mask
Users and physicians report these side effects from the use of a PAP mask: (1)
- Pressure on the cheekbones,
- dry oral and nasal mucous membranes (is alleviated by devices that can moisten the air we breathe),
- if the mask slips, the pressure cannot be maintained,
- Air in the abdomen, abdominal pain and flatulence,
- Eye irritation, dark circles and eye problems (when the mask slips and air escapes),
- it reduces and deconditions the natural force of the respiratory movement and can thus lead to impairments of breathing during the day, (2)
- Anxiety, panic attacks and claustrophobia, (3)
- Sore muscles in the chest,
- respiratory acidosis due to therapy (too little CO2 is exhaled),
- the sounds of the device can disturb the partner in bed (on the other hand, snoring is significantly reduced).
Sources
(1) Uniken Venema JAM, Knol-de Vries GE, van Goor H, Westra J, Hoekema A, Wijkstra PJ. Cardiovascular and metabolic effects of a mandibular advancement device and continuous positive airway pressure in moderate obstructive sleep apnea: a randomized controlled trial. J Clin Sleep Med. 2022 Jun 1; 18(6):1547-1555. doi: 10.5664/jcsm.9908. PMID: 35088708; PMCID: PMC9163609. – https://pubmed.ncbi.nlm.nih.gov/35088708/
(2) White DP, Shafazand S. Mandibular advancement device vs. CPAP in the treatment of obstructive sleep apnea: are they equally effective in Short term health outcomes? J Clin Sleep Med. 2013 Sep 15; 9(9):971-2. doi: 10.5664/jcsm.3008. PMID: 23997711; PMCID: PMC3746726. – https://pubmed.ncbi.nlm.nih.gov/23997711/
(3) Nocturnal breathing interruptions & CPAP mask robbed her of sleep – https://www.youtube.com/watch?v=-eCGHEi-iuY
CPAP / APAP - Differences
The advantages of APAP over CPAP include better patient compliance. It also facilitates individual fitting, making them a supplement or alternative to nightly laboratory titration studies. (1) There is also a difference in the costs: The statutory health insurance company only covers the costs of an APAP device if a medical prescription justifies the necessity with the ineffectiveness of classic CPAP therapy. (2) APAP and CPAP devices are very similar in terms of purchase price.
Sources
(1) Science Direct Positive Airway Pressure – https://www.sciencedirect.com/topics/medicine-and-dentistry/positive-airway-pressure
(2) MEOCLINIC Center for Snoring and Sleep Apnea – APAP – BPAP – CPAP – VPAP – what are the differences? – https://schlafapnoe-heilen.de/2019/08/30/apap-bpap-cpap-vpap-wo-liegen-die-unterschiede/
CPAP / APAP - Advantages
The breathing pressure adapts to the user's inhalation and exhalation rhythm. Most devices today offer a start-up function. This is intended to hinder the patient's falling asleep as little as possible. To do this, the pressure is slowly increased into the target area when falling asleep. The devices also often have air humidification, which is intended to prevent the mucous membranes from drying out.
The reviews at pubmed predominantly conclude that PAP therapy is more effective than oral aids in improving sleep-related breathing, as measured by the AHI value. The latter, on the other hand, are particularly popular with people with mild SAS and poor tolerance of PAP therapy. (1)
Sources
(1) Medical Advisory Secretariat. Oral appliances for obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser. 2009; 9(5):1-51. Epub 2009 Sep 1. PMID: 23074535; PMCID: PMC3377505. – https://pubmed.ncbi.nlm.nih.gov/23074535/
Hypoglossal stimulation
In hypoglossostimulation, the hypoglossos nerve is activated in a breath-synchronous manner via a pacemaker, thus pushing the tongue slightly forward during sleep. Doctors recommend using this therapy only with an AHI above 15 and with a body mass index (BMI) of no more than 32. It doesn't work if the narrowing/sagging affects the entire throat and not just the tongue. Otherwise, this procedure has quite good results. (1)(2)
Sources
(1) ENT guidebook: Sleep apnea syndrome: Alternatives to the mask – https://www.youtube.com/watch?v=qXYLKTpbeQA
(2) Nocturnal breathing interruptions & CPAP mask robbed her of sleep – https://www.youtube.com/watch?v=-eCGHEi-iuY
Grinding splint (s.a. CMD - craniomandibular dysfunction)
Health insurance companies
The costs for a snoring splint are only covered to a limited extent by health insurance companies. If you can prove that the snoring splint is medically absolutely necessary for you, the chances are good. If you suffer from sleep apnea, it is dangerous to your health. You can get confirmation of this from your doctor.
Life expectancy (see also sleep apnea syndrome – aging and life expectancy)
Lobbying
One example is the European Respiratory Society (ERS). It publishes guidelines for the treatment of SAS. Although they take into account all types of possible interventions, the PAP methods are always recommended as the first choice. (1)(2)(3) The long list of so-called "conflicts of interest", i.e. connections of members to manufacturers of PAP devices and the pharmaceutical industry, is impressive. (4)
Sources
(1) European Respiratory Society statement on sleep apnoea, sleepiness and driving risk
– https://erj.ersjournals.com/content/57/2/2001272
(2) European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnea – https://err.ersjournals.com/content/30/162/210200#sec-10
(3) Recommendations for the management of patients with obstructive sleep, apnea and hypertension – https://erj.ersjournals.com/content/41/3/523#sec-28
(4) Randerath W, Verbraecken J, de Raaff CAL, Hedner J, Herkenrath S, Hohenhorst W, Jakob T, Marrone O, Marklund M, McNicholas WT, Morgan RL, Pepin JL, Schiza S, Skoetz N, Smyth D, Steier J, Tonia T, Trzepizur W, van Mechelen PH, Wijkstra P. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur Respir Rev. 2021 Nov 30; 30(162):210200. doi: 10.1183/16000617.0200-2021 34853097. PMCID: PMC9489103. – https://pubmed.ncbi.nlm.nih.gov/34853097/
Medications: (see also sleep apnea syndrome – medications)
Operations
Surgery may be an option for moderate and severe forms of SAS. The most frequently performed operation internationally for the treatment of sleep apnea syndrome is an advance of the upper and lower jaw (maxillomandibular advancement). There are two types of advance displacement. According to the experience of scientists, the usual advance displacement corrects about 40% of sleep apnea. Extended surgery with even greater dilation of the airways can achieve a cure rate of up to 80%. (1)(2)(3)
In addition, there are the surgical variants in which the nose is changed, the tonsils are removed (tonsillectomy), the soft palate or the base of the tongue is reduced. Experts say that although the sleep situation changes positively, sleep apnea syndrome does not improve significantly. (4) Recently, medical professionals have been proposing combined airway and bariatric surgery (CABS) in obese individuals to improve both obesity and SAS. (5)
Sources
(1) Central sleep apnea syndrome – Dr. Ralf Siedenberg, https://schlafapnoe.de/blog/das-zentrale-schlafapnoe-syndrom-von-dr-ralf-siedenberg/
(2) Maxillo-mandibular advancement for the treatment of obstructive sleep apnea – https://www.zmk-aktuell.de/fachgebiete/aesthetik/story/das-maxillo-mandibulaere-advancement-zur-therapie-der-obstruktiven-schlafapnoe__10169.html
(3) Obstructive sleep apnea surgery as a solution – https://obstruktiveschlafapnoe.de/schlafapnoe-behandlung/schlafapnoe-operation/
(4) ENT guidebook: Sleep apnea syndrome: Alternatives to masks – https://www.youtube.com/watch?v=qXYLKTpbeQA
(5) Lin CC, Liu KH, Lee LA, Chuang LP, Lin YS, Hsin LJ, Lin WN, Chiang YT, Cheng WN, Li HY. Combined Airway and Bariatric Surgery (CABS) for Obstructive Sleep Apnea Patients with Morbid Obesity: A Comprehensive Alternative Preliminary Study. J Clin Med. 2022 Nov 29; 11(23):7078. doi: 10.3390/jcm11237078. PMID: 36498653; PMCID: PMC9738588. – https://pubmed.ncbi.nlm.nih.gov/36498653/
Sleep apnea syndrome (SAS)
Researchers distinguish between pure sleep-related breathing disorders, which have no or little immediate consequences for everyday life, and sleep apnea syndrome (SAS). Sleep apnea syndrome is the most common form of sleep-disordered breathing. (1) Experts distinguish between two forms: obstructive sleep apnea syndrome (mechanical cause, usually relaxation of the airway muscles) and central sleep apnea syndrome (due to disease of the central nervous system).
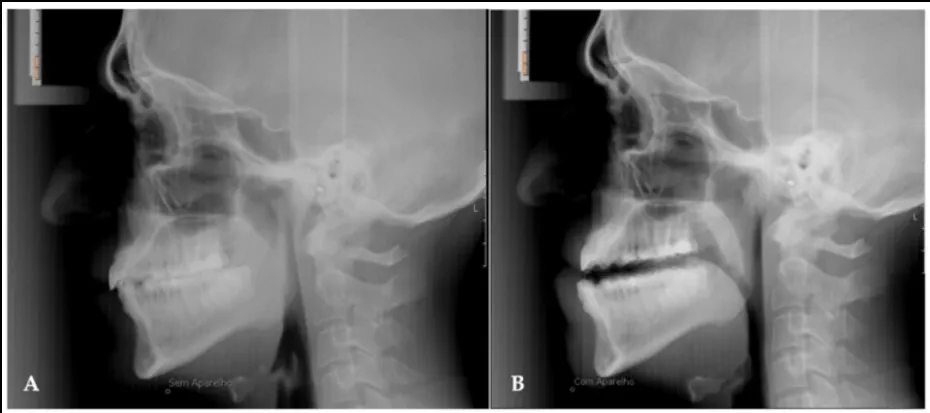
Cephalometric lateral image without protrusion splint (A) and one year after treatment with protrusion splint inserted (B).
Source: Life (Basel). 2022 Jun; 12(6): 835. Published online 2022 Jun 2. doi: 10.3390/life12060835
The main characteristics are apneas (respiratory arrests) and hypopneas (breathing restrictions) due to partial or complete closure of the airways. This leads to a recurring undersupply of oxygen in the body and especially in the brain. In response to the lack of oxygen, the affected person then inhales more intensively and noisily.
SAS is characterized by significant daytime sleepiness or even sleepiness (urgent need to sleep during the day or even acute microsleep). Today, it is undisputed that SAS is associated with a variety of comorbidities, an increase in mortality and sudden cardiac death. The more than twice as high risk of traffic accidents is mentioned less frequently. (see also Sleep apnea syndrome – Consequences II (road traffic))
Even though loud irregular snoring is considered one of the most common and characteristic symptoms of sleep apnea, it can also occur without the typical snoring sounds. This form is more likely to be found in women than in men.
Solutions used today include oral aids such as protrusion splints and tongue repositioning devices, PAP (Continuous/Automatic Positive Airway Pressure) machines, surgical procedures, hypoglossostimulation, drug therapies, positioning aids, and lifestyle changes. The two solutions that are mainly used are PAP machines and protrusion splints. The reviews at pubmed overwhelmingly conclude that PAP therapy is more effective in improving sleep-disordered breathing than any type of splints, as measured by the AHI value. The latter, on the other hand, are particularly popular with people with mild SAS and poor tolerance of PAP therapy. (2)
Read more about "CPAP / APAP – Disadvantages" and "CPAP / APAP – Health Benefits"
Sources
(1) Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993 Apr 29; 328(17):1230-5. doi: 10.1056/NEJM199304293281704. PMID: 8464434 – https://pubmed.ncbi.nlm.nih.gov/8464434/
(2) Medical Advisory Secretariat. Oral appliances for obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser. 2009; 9(5):1-51. Epub 2009 Sep 1. PMID: 23074535; PMCID: PMC3377505. – https://pubmed.ncbi.nlm.nih.gov/23074535/
Sleep apnea syndrome – aging and life expectancy
The negative effects of SAS on aging are not yet fully perceived by sufferers and medical professionals, as most know little about this complex disease and the number of undiagnosed cases is still quite high. (1) (see also sleep apnea syndrome – diagnosis)
Researchers suspect that SAS accelerates and intensifies aging. On the one hand, they justify this with the serious secondary diseases and on the other hand with the proven depletion of stem cells, wear and tear of the telomeres and epigenetic changes. (2)(3)
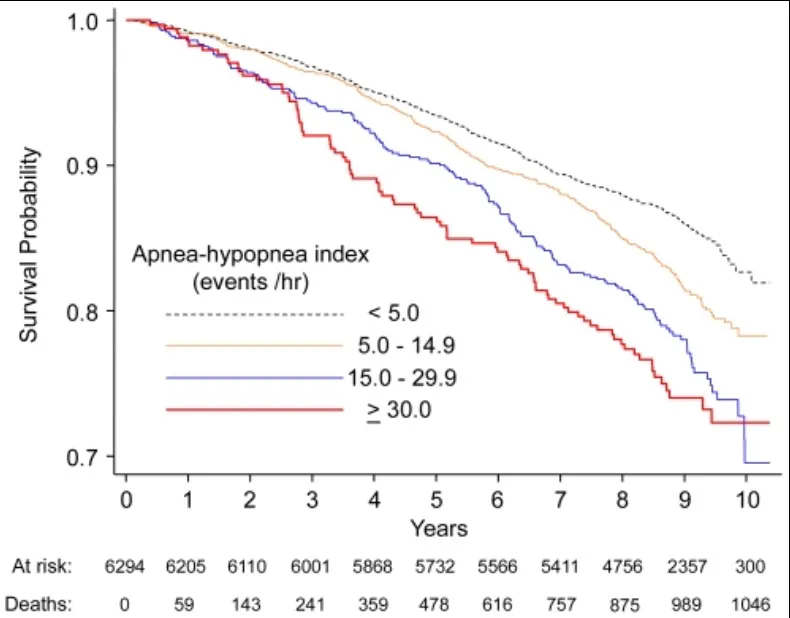
Kaplan-Meier survival curves as a function of different categories of apnea-hypopnea index and the duration of sleep apnea syndrome
Copyright: Punjabi et al. PLoS Med. 2009 Aug; 6(8): e1000132.
Sources
(1) Li Y, Wang Y. Obstructive Sleep Apnea-hypopnea Syndrome as a Novel Potential Risk for Aging. Aging Dis. 2021 Apr 1; 12(2):586-596. doi: 10.14336/AD.2020.0723. PMID: 33815884; PMCID: PMC7990365. – https://pubmed.ncbi.nlm.nih.gov/33815884/
(2) Gaspar LS, Álvaro AR, Moita J, Cavadas C. Obstructive Sleep Apnea and Hallmarks of Aging. Trends Mol Med. 2017 Aug; 23(8):675-692. doi: 10.1016/j.molmed.2017.06.006. Epub 2017 Jul 21 PMID: 28739207 – https://pubmed.ncbi.nlm.nih.gov/28739207/
(3) Turkiewicz S, Ditmer M, Sochal M, Białasiewicz P, Strzelecki D, Gabryelska A. Obstructive Sleep Apnea as an Acceleration Trigger of Cellular Senescence Processes through Telomere Shortening. Int J Mol Sci. 2021 Nov 21; 22(22):12536. doi: 10.3390/ijms222212536. PMID: 34830418; PMCID: PMC8624921. – https://pubmed.ncbi.nlm.nih.gov/34830418/
Sleep apnea syndrome – intestinal flora / leaky gut syndrome
Although the intricacies of the mechanisms leading to disease are not yet well understood, the available evidence suggests a link between obstructive sleep apnea and the composition of the microbiota in both directions. Sleep interruptions, recurring oxygen deprivation, and high levels of carbon dioxide all play an important role in changing the microbiome. Conversely, there are initial indications that changes in the microbiome influence sleep behavior. (1)(2)
One study looked at people with an AHI of more than 20 – the results: They have more Firmicutes, more bacteria that trigger inflammation and fewer bacteria (Bacteroides, Prevotella) that produce short-chain fatty acids. In short, sleep apnea promotes dysbiosis. (3) Researchers even found this change in the intestinal flora in children. (4) The occurrence of bacteria involved in the integrity of the intestinal barrier (Desulfovibrionaceae, Bacteroides fragilis and Faecalibacterium prausnitzii) differs significantly between children with and without SAS. (5)
For a few years now, there has also been the hypothesis that SAS and leaky gut syndrome are related, which is currently still being investigated. (6)(7)
Sources
(1) Cai Y, Juszczak HM, Cope EK, Goldberg AN. The microbiome in obstructive sleep apnea. Sleep. 2021 Aug 13; 44(8):ZSAB061. doi: 10.1093/sleep/zsab061. PMID: 33705556. – https://pubmed.ncbi.nlm.nih.gov/33705556/
(2) Durgan DJ. Obstructive Sleep Apnea-Induced Hypertension: Role of the Gut Microbiota. Curr Hypertens Rep. 2017 Apr; 19(4):35. doi: 10.1007/s11906-017-0732-3. PMID: 28365886 – https://pubmed.ncbi.nlm.nih.gov/28365886/
(3) Lu D, Xu S, Dai P, Wu L, Zhang H, Zhou B. Gut microbiota in hypertensive patients with versus without obstructive sleep apnea. J Clin Hypertens (Greenwich). 2022 Nov 21. doi: 10.1111/jch.14598. Epub ahead of print. PMID: 36411588 – https://pubmed.ncbi.nlm.nih.gov/36411588/
(4) Liu W, Du Q, Zhang H, Han D. The gut microbiome and obstructive sleep apnea syndrome in children. Sleep Med. 2022 Dec;100:462-471. doi: 10.1016/j.sleep.2022.09.022. Epub 2022 Sep 30 PMID: 36252415 – https://pubmed.ncbi.nlm.nih.gov/36252415/
(5) Valentini F, Evangelisti M, Arpinelli M, Di Nardo G, Borro M, Simmaco M, Villa MP. Gut microbiota composition in children with obstructive sleep apnea syndrome: a pilot study. Sleep Med. 2020 Dec;76:140-147. doi: 10.1016/j.sleep.2020.10.017. Epub 2020 Oct 17 PMID: 33181474 – https://pubmed.ncbi.nlm.nih.gov/33181474/
(6) Gawlik-Kotelnicka O, Margulska A, Gabryelska A, Sochal M, Białasiewicz P, Strzelecki D. "Leaky Gut" as a Keystone of the Connection between Depression and Obstructive Sleep Apnea Syndrome? A Rationale and Study Design. Metabolites. 2022 Feb 6; 12(2):152. doi: 10.3390/metabo12020152. PMID: 35208226; PMCID: PMC8878827. – https://pubmed.ncbi.nlm.nih.gov/35208226/
(7) Barceló A, Esquinas C, Robles J, Piérola J, De la Peña M, Aguilar I, Morell-Garcia D, Alonso A, Toledo N, Sánchez-de la Torre M, Barbé F. Gut epithelial barrier markers in patients with obstructive sleep apnea. Sleep Med. 2016 Oct;26:12-15. doi: 10.1016/j.sleep.2016.01.019. Epub 2016 Sep 28 PMID: 28007354 – https://pubmed.ncbi.nlm.nih.gov/28007354/
Sleep apnea syndrome – dementia, Alzheimer's disease
Studies reveal an area linked to SAS that surprises even experts. There is growing evidence of a link between cognitive decline and sleep-disordered breathing. Not only in the elderly, but also in middle-aged people. Researchers agree that mild cognitive impairment (MCI) is a consequence of SAS. (1) Interestingly, perception and memory are not affected. However, the mental limitation is evident in attention, the speed with which information can be processed, and conscious action and decision-making. (2)(3)
The positive news is that therapeutic measures to reduce SAS can stop and reverse this development. However, patience and adherence to therapy over a longer period of time are absolute prerequisites for this. (1)(4)(5)(6) However, this also implies the opposite: SAS that lasts for years and is not treated or treated inadequately increases the likelihood of dementia and Alzheimer's disease. (7)(8)(9) In addition to the lack of regeneration and the lack of oxygen at night, an overactivity of the sympathetic nervous system is suspected as a causative factor. (10)(11)(12)
Read more about "Sleep apnea syndrome – overactive sympathetic nervous system"
Sources
(1) Seda G, Matwiyoff G, Parrish JS. Effects of Obstructive Sleep Apnea and CPAP on Cognitive Function. Curr Neurol Neurosci Rep. 2021 May 6; 21(7):32. doi: 10.1007/s11910-021-01123-0. PMID: 33956247 – https://pubmed.ncbi.nlm.nih.gov/33956247/
(2) Leng Y, McEvoy CT, Allen IE, Yaffe K. Association of Sleep-Disordered Breathing with Cognitive Function and Risk of Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA Neurol. 2017 Oct 1; 74(10):1237-1245. doi: 10.1001/jamaneurol.2017.2180. Erratum in: JAMA Neurol. 2018 Jan 1; 75(1):133. PMID: 28846764; PMCID: PMC5710301. – https://pubmed.ncbi.nlm.nih.gov/28846764/
(3) Zhu X, Zhao Y. Sleep-disordered breathing and the risk of cognitive decline: a meta-analysis of 19,940 participants. Sleep Breath. 2018 Mar; 22(1):165-173. doi: 10.1007/s11325-017-1562-x. Epub 2017 Sep 13 PMID: 28905231 – https://pubmed.ncbi.nlm.nih.gov/28905231/
(4) Jiang X, Wang Z, Hu N, Yang Y, Xiong R, Fu Z. Cognition effectiveness of continuous positive airway pressure treatment in obstructive sleep apnea syndrome patients with cognitive impairment: a meta-analysis. Exp Brain Res. 2021 Dec; 239(12):3537-3552. doi: 10.1007/s00221-021-06225-2. Epub 2021 Sep 21 PMID: 34546386 – https://pubmed.ncbi.nlm.nih.gov/34546386/
(5) Wang G, Goebel JR, Li C, Hallman HG, Gilford TM, Li W. Therapeutic effects of CPAP on cognitive impairments associated with OSA. J Neurol. 2020 Oct; 267(10):2823-2828. doi: 10.1007/s00415-019-09381-2. Epub 2019 May 20. PMID: 31111204. – https://pubmed.ncbi.nlm.nih.gov/31111204/
(6) Fernandes M, Placidi F, Mercuri NB, Liguori C. The Importance of Diagnosing and the Clinical Potential of Treating Obstructive Sleep Apnea to Delay Mild Cognitive Impairment and Alzheimer's Disease: A Special Focus on Cognitive Performance. J Alzheimers Dis Rep. 2021 Jun 17; 5(1):515-533. doi: 10.3233/ADR-210004. PMID: 34368635; PMCID: PMC8293664. – https://pubmed.ncbi.nlm.nih.gov/34368635/
(7) Lal C, Ayappa I, Ayas N, Beaudin AE, Hoyos C, Kushida CA, Kaminska M, Mullins A, Naismith SL, Osorio RS, Phillips CL, Parekh A, Stone KL, Turner AD, Varga AW. The Link between Obstructive Sleep Apnea and Neurocognitive Impairment: An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2022 Aug; 19(8):1245-1256. doi: 10.1513/AnnalsATS.202205-380ST. PMID: 35913462; PMCID: PMC9353960. – https://pubmed.ncbi.nlm.nih.gov/35913462/
(8) Bubu OM, Andrade AG, Umasabor-Bubu OQ, Hogan MM, Turner AD, de Leon MJ, Ogedegbe G, Ayappa I, Jean-Louis G G, Jackson ML, Varga AW, Osorio RS. Obstructive sleep apnea, cognition and Alzheimer's disease: A systematic review integrating three decades of multidisciplinary research. Sleep Med Rev. 2020 Apr;50:101250. doi: 10.1016/j.smrv.2019.101250. Epub 2019 Dec 12. PMID: 31881487; PMCID: PMC7593825. – https://pubmed.ncbi.nlm.nih.gov/31881487/
(9) Liguori C, Maestri M, Spanetta M, Placidi F, Bonanni E, Mercuri NB, Guarnieri B. Sleep-disordered breathing and the risk of Alzheimer's disease. Sleep Med Rev. 2021 Feb;55:101375. doi: 10.1016/j.smrv.2020.101375. Epub 2020 Sep 6 PMID: 33022476 – https://pubmed.ncbi.nlm.nih.gov/33022476/
(10) Herberts M, Kolla B, Paul T, Mekala P, Mansukhani MP. Sleep apnea and autonomic dysfunction in patients with dementia. Front Neurosci. 2022 Nov 3;16:951147. doi: 10.3389/fnins.2022.951147. PMID: 36408398; PMCID: PMC9669746. – https://pubmed.ncbi.nlm.nih.gov/36408398/
(11) Dräger LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstructive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. J Am Coll Cardiol. 2013 Aug 13; 62(7):569-76. doi: 10.1016/j.jacc.2013.05.045. Epub 2013 Jun 12. PMID: 23770180; PMCID: PMC4461232. – https://pubmed.ncbi.nlm.nih.gov/23770180/
(12) Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995 Oct; 96(4):1897-904. doi: 10.1172/JCI118235. PMID: 7560081; PMCID: PMC185826. – https://pubmed.ncbi.nlm.nih.gov/7560081/
Sleep apnea syndrome – high blood pressure
One of the most common side effects of sleep apnea is increased blood pressure. At night, SAS patients very often have significantly increased blood pressure compared to healthy individuals. This also shows significant fluctuations that can be reconciled with the course of apnea. In individual cases, researchers were able to determine peak values of 240/130 mmHg. (1) It is particularly striking that high blood pressure persists in many people during the day. The cause seems to be not only respiratory arrest and lack of oxygen, but also similarly increased sympathetic activity.
Read more about "Sleep apnea syndrome – overactive sympathetic nervous system"
Sources
(1) Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995 Oct; 96(4):1897-904. doi: 10.1172/JCI118235. PMID: 7560081; PMCID: PMC185826. – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC185826/?page=2
Sleep apnea syndrome – diabetes
SAS exacerbates the already critical metabolic situation in many affected persons (metabolic syndrome) in a way that is still unclear. In addition to the effects mentioned above, such as high blood pressure, aging, mental decline, researchers were also able to demonstrate a correlation between impaired sugar metabolism or insulin resistance and SAS. (1)(2)(3)
In their paper entitled "Sleep apnea is a manifestation of the metabolic syndrome", the researchers Vgontzas, Bixler and Chrousos give several reasons that pro-inflammatory cytokines (Il-6, TNF-alpha) and insulin resistance are the mediators of greatly increased daytime sleepiness and sleep apnea. (4)
Sources
(1) Azman M, Sani A, Kamaruddin NA. Insulin resistance using HOMA model in obstructive sleep apnea: a cross sectional study. Ann Saudi Med. 2014 Nov-Dec; 34(6):476-81. doi: 10.5144/0256-4947.2014.476 25971819. PMCID: PMC6074568. – https://pubmed.ncbi.nlm.nih.gov/25971819/
(2) Ip MS, Lam B, Ng MM, Lam WK, Tsang KW, Lam KS. Obstructive sleep apnea is independently associated with insulin resistance. Am J Respir Crit Care Med. 2002 Mar 1; 165(5):670-6. doi: 10.1164/ajrccm.165.5.2103001. PMID: 11874812 – https://pubmed.ncbi.nlm.nih.gov/11874812/
(3) Protasiewicz Timofticiuc DC, Vladu IM, Ștefan AG, Clenciu D, Mitrea A, Pădureanu V, Efrem IC, Diaconu ID, Turcu A, Țenea-Cojan TȘ, Hâncu AM, Forțofoiu M, Mirea Munteanu O, Moța M. Associations of Chronic Diabetes Complications and Cardiovascular Risk with the Risk of Obstructive Sleep Apnea in Patients with Type 2 Diabetes. J Clin Med. 2022 Jul 28; 11(15):4403. doi: 10.3390/jcm11154403. PMID: 35956020; PMCID: PMC9368962 – https://pubmed.ncbi.nlm.nih.gov/35956020/
(4) Vgontzas AN, Bixler EO, Chrousos GP. Sleep apnea is a manifestation of the metabolic syndrome. Sleep Med Rev. 2005 Jun; 9(3):211-24. doi: 10.1016/j.smrv.2005.01.006. PMID: 15893251. – https://pubmed.ncbi.nlm.nih.gov/15893251/
Sleep apnea syndrome – Diagnosis
A study from 2022 indicates six variables that allowed a very good prediction for the SAS. These are: high body mass index (BMI), high blood pressure, dry mouth in the morning, waking up at night after breathing interruptions, witnessed apnea and the ESS total score (questionnaire "Epworth Sleepiness Scale"). (1) Self-diagnosis is made more difficult because those affected usually do not remember the breathing interruptions. The respiratory arrests usually do not lead to complete awakening. Subjectively, there is no reason for the increased daytime sleepiness. People with few apneas and/or hypopneas are often not significantly more tired than usual during the day, which means that they are usually unaware of their breathing disorders. (2) Therefore, the above-mentioned factors are often the indications, or should be, that give rise to an examination for sleep apnea.
Sources
(1) Yan X, Wang L, Liang C, Zhang H, Zhao Y, Zhang H, Yu H, Di J. Development and assessment of a risk prediction model for moderate-to-severe obstructive sleep apnea. Front Neurosci. 2022 Aug 5;16:936946. doi: 10.3389/fnins.2022.936946. PMID: 35992917; PMCID: PMC9390335. – https://pubmed.ncbi.nlm.nih.gov/35992917/
(2) Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993 Apr 29; 328(17):1230-5. doi: 10.1056/NEJM199304293281704. PMID: 8464434 – https://pubmed.ncbi.nlm.nih.gov/8464434/
Sleep apnea syndrome - frequency
50 years ago, when the first studies on sleep apnea syndrome (SAS) were published, patients still had to be laboriously gathered. Today, it is widespread and is considered a progressive, chronic disease. (1) The figures on how many people are (probably) affected by sleep apnea syndrome in Germany vary greatly, depending on the source. The minimum estimates are one to two percent of women and two to four percent of men aged 40 and over. (2)(3) The maximum estimates are 13% of women and 25 to 30% of men. (4)(5)
In studies that deal with the prevalence, the criteria, age groups and people involved are often quite different. Therefore, there are large differences in values. According to figures from the Wisconsin Sleep Cohort Study, in 2010, 10% of Americans aged 30 to 49 and 17% between the ages of 50 and 70 were affected. Among women, the figures were 3% and 9% respectively. (6) A study in Saudi Arabia came to a frequency of almost 27% – with an average age of 30 years! (7)
The change in frequencies with age is interesting. As expected, the mild forms of SAS and sleep-related breathing disorders are significantly more common in the age group under 60 years than the moderate and severe forms. There are very few severe forms among women in this age range. It is striking that in men in the age group of 60 years and older, SAS in the moderate or severe form is just as common as the mild form. So the severe form increases significantly with age. (8) An Australian study found a peak of 49% for people with moderate or severe sleep apnea at an older age. (9) The increase in numbers over the last 20 years is also due to the increased sensitivity of the measurement technology used and changed criteria for diagnosing sleep apnea.A study from 2022 indicates six variables that allowed a very good prediction of SAS. These are: high body mass index (BMI), high blood pressure, dry mouth in the morning, waking up at night after breathing interruptions, witnessed apnea and the ESS total score (questionnaire "Epworth Sleepiness Scale"). (1) Self-diagnosis is made more difficult because those affected usually do not remember the breathing interruptions. The respiratory arrests usually do not lead to complete awakening. Subjectively, there is no reason for the increased daytime sleepiness. People with few apneas and/or hypopneas are often not significantly more tired than usual during the day, which means that they are usually unaware of their breathing disorders. (2) Therefore, the above-mentioned factors are often the indications, or should be, that give rise to an examination for sleep apnea.
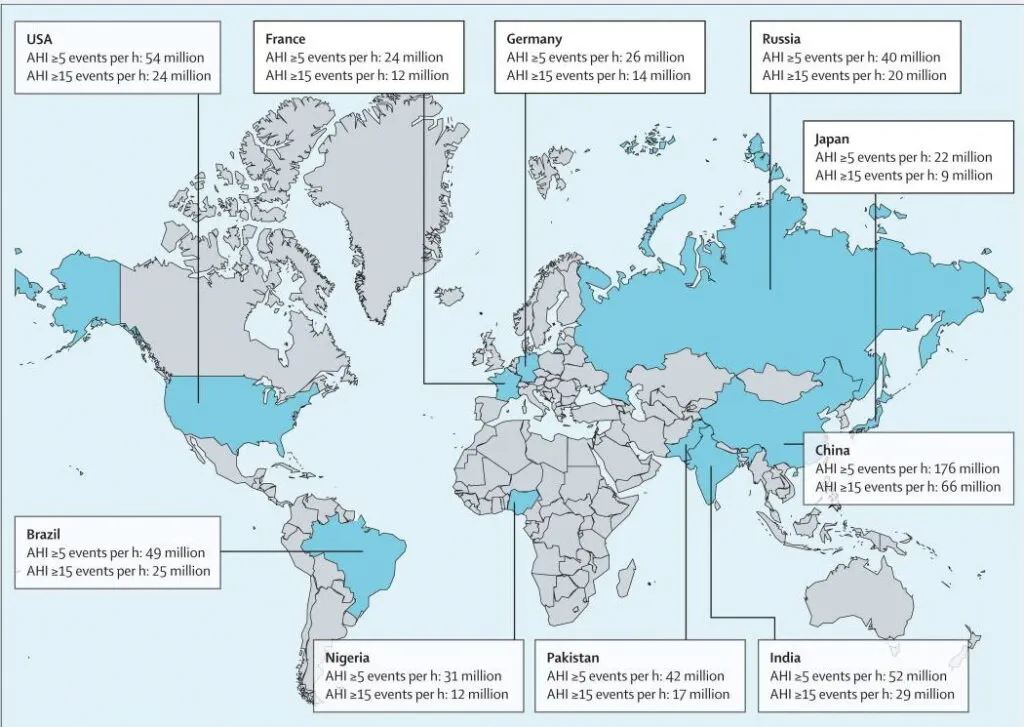
The ten countries with the highest estimated number of people with obstructive sleep apnea according to the criteria of the American Academy of Sleep Medicine 2012
Image Source: Lancet Respir Med. 2019 Aug; 7(8): 687–698. Published online 2019 Jul 9. doi: 10.1016/S2213-2600(19)30198-5
Sources
(1) Ferran Barbé, Jean-Louis Pépin: "Obstructive Sleep Apnea" – https://books.ersjournals.com/content/obstructive-sleep-apnoea
(2) Brochure of the SHG Sleep Apnea District Bergstraße
(3) Medical Advisory Secretariat. Polysomnography in patients with obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser. 2006; 6(13):1-38. Epub 2006 Jun 1. PMID: 23074483; PMCID: PMC3379160. – https://pubmed.ncbi.nlm.nih.gov/23074483/
(4) Sleep apnea bti Human Technology – https://bti-biotechnologyinstitute.com/de/losungen-und-produkte/schlafapnoe
(5) Akset M, Poppe KG, Kleynen P, Bold I, Bruyneel M. Endocrine disorders in obstructive sleep apnoea syndrome: A bidirectional relationship. Clin Endocrinol (Oxf). 2022 Feb 19. doi: 10.1111/cen.14685. Epub ahead of print. PMID: 35182448 – https://pubmed.ncbi.nlm.nih.gov/35182448/
(6) Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013 May 1; 177(9):1006-14. doi: 10.1093/aje/kws342. Epub 2013 Apr 14. PMID: 23589584; PMCID: PMC3639722. – https://pubmed.ncbi.nlm.nih.gov/23589584/
(7) Alsultan A, Al Sahlawi M, Agha M. Prevalence of Obstructive Sleep Apnea Symptoms Among the Adult Population in Al-Ahsa, Saudi Arabia. Cureus. 2022 Nov 4; 14(11):E31082. doi: 10.7759/cureus.31082. PMID: 36475116; PMCID: PMC9719609. – https://pubmed.ncbi.nlm.nih.gov/36475116/
(8) Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, Mooser V, Preisig M, Malhotra A, Waeber G, Vollenweider P, Tafti M, Haba-Rubio J. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015 Apr; 3(4):310-8. doi: 10.1016/S2213-2600(15)00043-0. Epub 2015 Feb 12 25682233. PMCID: PMC4404207. – https://pubmed.ncbi.nlm.nih.gov/25682233/
(9) Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, Hamilton GS, Dharmage SC. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017 Aug;34:70-81. doi: 10.1016/j.smrv.2016.07.002. Epub 2016 Jul 18. PMID: 27568340. – https://pubmed.ncbi.nlm.nih.gov/27568340/
Sleep apnea syndrome – serious consequences I
Sleep-related breathing disorders have a number of health-critical consequences. The most threatening thing is the higher rate of illness and mortality. (1) All people with SAS experience a more or less severe impairment of sleep and recovery, which in itself is an increased risk of further ailments and chronic diseases. Due to the frequent almost waking up, the physiological sleep structure is permanently disturbed and the oxygen saturation of the blood decreases significantly. (2)(3) A lack of oxygen leads to negative adaptations in the metabolism via epigenetic mechanisms and thus to chronic diseases. (4)(5)
It is debated whether sleep apnea syndrome can cause other diseases. In any case, weight loss in obesity led to an 85.7% decrease in sleep apnea syndrome. Therefore, some scientists suspect that the often associated diseases such as high blood pressure and diabetes mellitus are mainly consequences of obesity and not SAS. (6)(7) (see also sleep apnea syndrome – high blood pressure and sleep apnea syndrome – diabetes)
On the other hand, the figures are quite clear for stroke, coronary heart disease, heart failure, cancer and premature mortality. (8)(9)(10)(11)(12)(13)(14)(15)(16)(17) However, the associations with heart disease have been established in people with SAS who are not undergoing therapy and have not yet used any aids. Study data suggest accelerated vascular aging in individuals at high risk of SAS. This could be at least partly the cause of the increased incidence of cardiovascular diseases. (18)
Hardly anyone expects a different correlation: Researchers found a relationship between SAS or sleep-related breathing disorders in childhood and behavioral changes, growth disorders or poorer school grades, and lower academic performance in adulthood. (19)(20)(21)(22)
Sources
(1) Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobbäck N, Mooser V, Preisig M, Malhotra A, Waeber G, Vollenweider P, Tafti M, Haba-Rubio J. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015 Apr; 3(4):310-8. doi: 10.1016/S2213-2600(15)00043-0. Epub 2015 Feb 12 25682233. PMCID: PMC4404207. – https://pubmed.ncbi.nlm.nih.gov/25682233/
(2) Sleep apnea syndrome – https://de.wikipedia.org/wiki/Schlafapnoe-Syndrom
(3) Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, D'Agostino RB, Newman AB, Lebowitz MD, Pickering TG. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000 Apr 12; 283(14):1829-36. doi: 10.1001/jama.283.14.1829. Erratum in: JAMA 2002 Oct 23-30; 288(16):1985. PMID: 10770144 – https://pubmed.ncbi.nlm.nih.gov/10770144/
(4) Cheung EC, Kay MW, Schunke KJ. Epigenetic Alterations in Pediatric Sleep Apnea. Int J Mol Sci. 2021 Sep 1; 22(17):9523. doi: 10.3390/ijms22179523. PMID: 34502428; PMCID: PMC8430725. – https://pubmed.ncbi.nlm.nih.gov/34502428/
(5) Chen YC, Hsu PY, Hsiao CC, Lin MC. Epigenetics: A Potential Mechanism Involved in the Pathogenesis of Various Adverse Consequences of Obstructive Sleep Apnea. Int J Mol Sci. 2019 Jun 15; 20(12):2937. doi: 10.3390/ijms20122937. PMID: 31208080; PMCID: PMC6627863. – https://pubmed.ncbi.nlm.nih.gov/31208080/
(6) Medical Advisory Secretariat. Polysomnography in patients with obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser. 2006; 6(13):1-38. Epub 2006 Jun 1. PMID: 23074483; PMCID: PMC3379160. – https://pubmed.ncbi.nlm.nih.gov/23074483/
(7) O'Connor GT, Caffo B, Newman AB, Quan SF, Rapoport DM, Redline S, Resnick HE, Samet J, Shahar E. Prospective study of sleep-disordered breathing and hypertension: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2009 Jun 15; 179(12):1159-64. doi: 10.1164/rccm.200712-1809OC. Epub 2009 Mar 5. PMID: 19264976; PMCID: PMC2695498. – https://pubmed.ncbi.nlm.nih.gov/19264976/
(8) Arzt M, Young T, Finn L, Skatrud JB, Bradley TD. Association of sleep-disordered breathing and the occurrence of stroke. Am J Respir Crit Care Med. 2005 Dec 1; 172(11):1447-51. doi: 10.1164/rccm.200505-702OC. Epub 2005 Sep 1. PMID: 16141444; PMCID: PMC2718439. – https://pubmed.ncbi.nlm.nih.gov/16141444/
(9) Hla KM, Young T, Hagen EW, Stein JH, Finn LA, Nieto FJ, Peppard PE. Coronary heart disease incidence in sleep disordered breathing: the Wisconsin Sleep Cohort Study. Sleep. 2015 May 1; 38(5):677-84. doi: 10.5665/sleep.4654. PMID: 25515104; PMCID: PMC4402672. – https://pubmed.ncbi.nlm.nih.gov/25515104/
(10) Gottlieb DJ, Yenokyan G, Newman AB, O'Connor GT, Punjabi NM, Quan SF, Redline S, Resnick HE, Tong EK, Diener-West M, Shahar E. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation. 2010 Jul 27; 122(4):352-60. doi: 10.1161/CIRCULATIONAHA.109.901801. Epub 2010 Jul 12. PMID: 20625114; PMCID: PMC3117288. – https://pubmed.ncbi.nlm.nih.gov/20625114/
(11) Punjabi NM, Caffo BS, Goodwin JL, Gottlieb DJ, Newman AB, O'Connor GT, Rapoport DM, Redline S, Resnick HE, Robbins JA, Shahar E, Unruh ML, Samet JM. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009 Aug; 6(8):E1000132. doi: 10.1371/journal.pmed.1000132. Epub 2009 Aug 18. PMID: 19688045; PMCID: PMC2722083. – https://pubmed.ncbi.nlm.nih.gov/19688045/
(12) Nieto FJ, Peppard PE, Young T, Finn L, Hla KM, Farré R. Sleep-disordered breathing and cancer mortality: results from the Wisconsin Sleep Cohort Study. Am J Respir Crit Care Med. 2012 Jul 15; 186(2):190-4. doi: 10.1164/rccm.201201-0130OC. Epub 2012 May 20. PMID: 22610391; PMCID: PMC3406081. – https://pubmed.ncbi.nlm.nih.gov/22610391/
(13) Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, Stubbs R, Hla KM. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008 Aug; 31(8):1071-8. PMID: 18714778; PMCID: PMC2542952. – https://pubmed.ncbi.nlm.nih.gov/18714778/
(14) Kendzerska T, Mollayeva T, Gershon AS, Leung RS, Hawker G, Tomlinson G. Untreated obstructive sleep apnea and the risk for serious long-term adverse outcomes: a systematic review. Sleep Med Rev. 2014 Feb; 18(1):49-59. doi: 10.1016/j.smrv.2013.01.003. Epub 2013 May 1. PMID: 23642349. – https://pubmed.ncbi.nlm.nih.gov/23642349/
(15) Palamaner Subash Shantha G, Kumar AA, Cheskin LJ, Pancholy SB. Association between sleep-disordered breathing, obstructive sleep apnea, and cancer incidence: a systematic review and meta-analysis. Sleep Med. 2015 Oct; 16(10):1289-94. doi: 10.1016/j.sleep.2015.04.014. Epub 2015 May 22 PMID: 26212231 – https://pubmed.ncbi.nlm.nih.gov/26212231/
(16) Cheng H, Li D. Investigation into the association between obstructive sleep apnea and incidence of all-type cancers: a systematic review and meta-analysis. Sleep Med. 2021 Dec;88:274-281. doi: 10.1016/j.sleep.2021.05.031. Epub 2021 Jun 4. PMID: 34219029. – https://pubmed.ncbi.nlm.nih.gov/34219029/
(17) Xiong H, Lao M, Wang L, Xu Y, Pei G, Lu B, Shi Q, Chen J, Zhang S, Ou Q. The Incidence of Cancer Is Increased in Hospitalized Adult Patients With Obstructive Sleep Apnea in China: A Retrospective Cohort Study. Front Oncol. 2022 Mar 31;12:856121. doi: 10.3389/fonc.2022.856121. PMID: 35433429; PMCID: PMC9008763. – https://pubmed.ncbi.nlm.nih.gov/35433429/
(18) Lisan Q, van Sloten T, Boutouyrie P, Laurent S, Danchin N, Thomas F, Guibout C, Perier MC, Dagnelie P, Henry RM, Schram MT, Heinzer R, Marques-Vidal P, van der Kallen CJ, Crijns HJ, van Greevenbroek M, Reesink K, Köhler S, Sastry M, Jouven X, Stehouwer CDA, Empana JP. Sleep Apnea is Associated With Accelerated Vascular Aging: Results From 2 European Community-Based Cohort Studies. J Am Heart Assoc. 2021 Aug 3; 10(15):E021318. doi: 10.1161/JAHA.120.021318. Epub 2021 Jul 26 PMID: 34308679; PMCID: PMC8475690. – https://pubmed.ncbi.nlm.nih.gov/34308679/
(19) Nosetti L, Zaffanello M, Katz ES, Vitali M, Agosti M, Ferrante G, Cilluffo G, Piacentini G, La Grutta S. Twenty-year follow-up of children with obstructive sleep apnea. J Clin Sleep Med. 2022 Jun 1; 18(6):1573-1581. doi: 10.5664/jcsm.9922. PMID: 35164899; PMCID: PMC9163630. – https://pubmed.ncbi.nlm.nih.gov/35164899/
(20) Torres-López LV, Cadenas-Sanchez C, Migueles JH, Esteban-Cornejo I, Molina-Garcia P, H Hillman C, Catena A, Ortega FB. Does sleep-disordered breathing add to impairments in academic performance and brain structure usually observed in children with overweight/obesity? Eur J Pediatr. 2022 May; 181(5):2055-2065. DOI: 10.1007/s00431-022-04403-0. Epub 2022 Feb 10 PMID: 35142932; PMCID: PMC9056447. – https://pubmed.ncbi.nlm.nih.gov/35142932/
(21) Ezeugwu VE, Adamko D, van Eeden C, Dubeau A, Turvey SE, Moraes TJ, Simons E, Subbarao P, Wishart DS, Mandhane PJ. Development of a predictive algorithm to identify pre-school children at risk for behavior changes associated with sleep-related breathing disorders. Sleep Med. 2022 Dec;100:472-478. doi: 10.1016/j.sleep.2022.09.015. Epub 2022 Sep 24 PMID: 36252416 - https://pubmed.ncbi.nlm.nih.gov/36252416/
(22) Guard AJB, Gibson NA, Samuels MP, Evans HJ. Recent advances in paediatric sleep disordered breathing. Breathe (Sheff). 2022 Sep; 18(3):220151. doi: 10.1183/20734735.0151-2022. Epub 2022 Oct 11 36340818. PMCID: PMC9584598. – https://pubmed.ncbi.nlm.nih.gov/36340818/
Sleep apnea syndrome – serious consequences II (road traffic)
Obstructive sleep apnea is the most common medical cause of excessive daytime sleepiness. In terms of safety when driving, the spontaneous tendency to fall asleep is a major problem that leads to a more than twice the risk of traffic accidents. (1) In 2000, more than 800,000 drivers with SAS were involved in accidents in the United States. These cost 15.9 billion dollars and 1,400 lives this year. In the United States, medical treatment for all drivers suffering from SAS would cost $3.18 billion annually, save $11.1 billion in accident costs, and save 980 lives. (2) A Japanese study confirmed that both excessive daytime sleepiness and the severity of SAS are independently associated with the occurrence of road accidents. (3)
Sources
(1) Garbarino S. Excessive daytime sleepiness in obstructive sleep apnea: implications for driving licenses. Sleep Breath. 2020 Mar; 24(1):37-47. doi: 10.1007/s11325-019-01903-6. Epub 2019 Jul 24. PMID: 31342234. – https://pubmed.ncbi.nlm.nih.gov/31342234/
(2) Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep. 2004 May 1; 27(3):453-8. doi: 10.1093/sleep/27.3.453. PMID: 15164898. – https://pubmed.ncbi.nlm.nih.gov/15164898/
(3) Komada Y, Nishida Y, Namba K, Abe T, Tsuiki S, Inoue Y. Elevated risk of motor vehicle accident for male drivers with obstructive sleep apnea syndrome in the Tokyo metropolitan area. Tohoku J Exp Med. 2009 Sep; 219(1):11-6. doi: 10.1620/tjem.219.11. PMID: 19713679. – https://pubmed.ncbi.nlm.nih.gov/19713679/
Sleep apnea syndrome – hypothyroidism
Some studies describe a link between thyroid disease and SAS. Compared to the general population, the prevalence of SAS is increased in patients with obesity and hypothyroidism. It has not yet been clarified whether there is a direct link between SAS and thyroid disorders or whether it is indirectly related to obesity. (1)(2)(3)
Sources
(1) Pancholi C, Chaudhary SC, Gupta KK, Sawlani KK, Verma SK, Singh A, Verma AK, Usman K, Atam V. Obstructive sleep apnea in hypothyroidism. Ann Afr Med. 2022 Oct-Dec; 21(4):403-409. doi: 10.4103/aam.aam_134_21. PMID: 36412342. – https://pubmed.ncbi.nlm.nih.gov/36412342/
(2) Akset M, Poppe KG, Kleynen P, Bold I, Bruyneel M. Endocrine disorders in obstructive sleep apnoea syndrome: A bidirectional relationship. Clin Endocrinol (Oxf). 2022 Feb 19. doi: 10.1111/cen.14685. Epub ahead of print. PMID: 35182448 – https://pubmed.ncbi.nlm.nih.gov/35182448/
(3) Zhang M, Zhang W, Tan J, Zhao M, Zhang Q, Lei P. Role of hypothyroidism in obstructive sleep apnea: a meta-analysis. Curr Med Res Opin. 2016 Jun; 32(6):1059-64. doi: 10.1185/03007995.2016.1157461. Epub 2016 Mar 24 https://pubmed.ncbi.nlm.nih.gov/26907534/ 26907534.
Sleep apnea syndrome – children
Snoring and SAS are so common in children that it has long been impossible to speak of isolated cases. (1)(2)(3)(4)(5)(6) Figures on prevalence are very rare. One source reports 2 to 3 percent of the children. (7)
Adenotonsillectomy (removal of the palatine tonsils) is the first-line treatment for children with SAS. Recent findings show that intracapsular tonsillectomy leads to a lower rate of adverse events than conventional procedures. Dutch researchers show concerns about this method: Up to the age of 5, they could not detect any benefit from tonsillectomyng, and in about half of the children who did not undergo surgery, sleep patterns normalized within seven months. (8)
Anti-inflammatory drugs and support for breathing with positive airway pressure are not always appropriate or successful. Weight loss and stimulation of the hypoglossal nerve, on the other hand, can help. (6)(9)(10)
Sources
(1) Benbir Senel G, Aktan Suzgun M, Bibinoglu Amirov C, Karadeniz D. The Comparison of the Sleep Structure and Sleep Spindle Activity in Children With Primary Snoring and Sleep-Disordered Breathing. Clin Pediatr (Phila). 2022 Nov 25:99228221139985. doi: 10.1177/00099228221139985. Epub ahead of print. PMID: 36433642. – https://pubmed.ncbi.nlm.nih.gov/36433642/
(2) Bozzini MF, Di Francesco RC, Soster LA. Clinical and anatomical characteristics associated with obstructive sleep apnea severity in children. Clinics (Sao Paulo). 2022 Nov 1;77:100131. doi: 10.1016/j.clinsp.2022.100131. PMID: 36334493; PMCID: PMC9636441. – https://pubmed.ncbi.nlm.nih.gov/36334493/
(3) Kaditis AG, Alonso Alvarez ML, Boudewyns A, Alexopoulos EI, Ersu R, Joosten K, Larramona H, Miano S, Narang I, Trang H, Tsaoussoglou M, Vandenbussche N, Villa MP, Van Waardenburg D, Weber S, Verhulst S. Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J. 2016 Jan; 47(1):69-94. doi: 10.1183/13993003.00385-2015. Epub 2015 Nov 5. PMID: 26541535 – https://pubmed.ncbi.nlm.nih.gov/26541535/
(4) Krzeski A, Burghard M. Obstructive sleep disordered breathing in children – an important problem in the light of current European guidelines. Otolaryngol Pol. 2018 Jun 29; 72(5):9-16. doi: 10.5604/01.3001.0012.1570. PMID: 30460910. – https://pubmed.ncbi.nlm.nih.gov/30460910/
(5) Magnusdottir S, Witmans M, Hilmisson H. Sleep quality, sleep apnea, and metabolic health in children treated with adenotonsillectomy. Sleep Breath. 2022 Nov 24. doi: 10.1007/s11325-022-02747-3. Epub ahead of print. PMID: 36434376 – https://pubmed.ncbi.nlm.nih.gov/36434376/
(6) Guard AJB, Gibson NA, Samuels MP, Evans HJ. Recent advances in paediatric sleep disordered breathing. Breathe (Sheff). 2022 Sep; 18(3):220151. doi: 10.1183/20734735.0151-2022. Epub 2022 Oct 11 36340818. PMCID: PMC9584598. – https://pubmed.ncbi.nlm.nih.gov/36340818/
(7) Childhood asthma improves after adenotonsillectomy – https://medical-diag.com/7928-children-s-asthma-found-to-improve-after-adenotonsillectomy
(8) Venekamp RP, Hearne BJ, Chandrasekharan D, Blackshaw H, Lim J, Schilder AG. Tonsillectomy or adenotonsillectomy versus non-surgical management for obstructive sleep-disordered breathing in children. Cochrane Database Syst Rev. 2015 Oct 14; 2015(10):CD011165. doi: 10.1002/14651858.CD011165.pub2. PMID: 26465274; PMCID: PMC9242010. – https://pubmed.ncbi.nlm.nih.gov/26465274/
(9) Adenotonsillectomy for the treatment of severe obstructive sleep apnea in children with trisomy 21? – https://www.neuromedizin.de/Neurologie/Adenotonsillektomie-zur-Therapie-der-schweren-obstruktiven-S.htm
(10) Obstructive sleep apnea in children -https://www.msdmanuals.com/de-de/profi/lungenkrankheiten/schlafapnoe/obstruktive-schlafapnoe-bei-kindern
Sleep apnea syndrome – medication (cause and therapy)
Cause: Breathing reduction and pauses in breathing can be caused by some medications, including opioids, sleeping pills, sleep-inducing antidepressants and all other medications that lead to calming via the nervous system. When people are given medication for insomnia, there is a vicious circle that every doctor should know about. For the treatment of most sleep disorders, whether chronic or acute insomnia, the Z-drugs (zaleplon, zopiclone, zolpidem) and benzodiazepines are still the first choice. (1) Apart from the severe side effects and the accompanying addiction potential, these drugs are muscle relaxants and can thus contribute directly to sleep apnea syndrome. (2)(3)
Therapy: Currently (end of 2022), no drug therapy is routinely used for obstructive sleep apnea. Due to minor successes, the combination of noradrenergic (antidepressants) agents and muscarinic receptor antagonists is the focus of research. (4) The active ingredient atomoxetine (selective norepinephrine reuptake inhibitor, indication: attention deficit/hyperactivity disorder) alone and in combination with oxybutynin (antispasmodic/muscarinic receptor antagonist, indications: urinary incontinence, urge to urinate, overactive bladder) led to an improvement in the AHI and the oxygen saturation index in the mild form of SAS. At the same time, however, it also led to increased sleep disorders. (5) Other studies showed little or no improvement. (6)(7)(8)(9) Overall, however, the value of these studies is questionable, as they are single-dose experiments, i.e. each drug or drug combination was given only once and the effects were tracked for only one night.
In initial studies with the anti-dementia drug donepezil and the glucocorticoid fluticasone, there were indications of positive results, even if the mechanism of action is still unknown. (10) A comparative study collected the results of some sedatives and hypnotics. Above all, the authors note that there was no deterioration in the AHI and oxygen desaturation index (ODI). However, due to the limited data, they advise caution in prescribing such active ingredients for patients with SAS. (11)
Sources
(1) Tandon VR, Sharma S, Mahajan A, Mahajan A, Tandon A. Menopause and Sleep Disorders. J Midlife Health. 2022 Jan-Mar; 13(1):26-33. doi: 10.4103/jmh.jmh_18_22. Epub 2022 May 2 35707298. PMCID: PMC9190958. – https://pubmed.ncbi.nlm.nih.gov/35707298/
(2) https://de.wikipedia.org/wiki/Benzodiazepine
(3) https://de.wikipedia.org/wiki/Zopiclon
(4) Zha S, Yang H, Yue F, Zhang Q, Hu K. Combined noradrenergic plus antimuscarinic agents for obstructive sleep apnea – A systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2022 Aug;64:101649. doi: 10.1016/j.smrv.2022.101649. Epub 2022 May 28 PMID: 35709641 – https://pubmed.ncbi.nlm.nih.gov/35709641/
(5) Schweitzer PK, Maynard JP, Wylie PE, Emsellem HA, Sands SA. Efficacy of atomoxetine plus oxybutynin in the treatment of obstructive sleep apnea with moderate pharyngeal collapsibility. Sleep Breath. 2022 May 13:1–9. doi: 10.1007/s11325-022-02634-x. Epub ahead of print. PMID: 35551600; PMCID: PMC9098382. – https://pubmed.ncbi.nlm.nih.gov/35551600/
(6) Aishah A, Lim R, Sands SA, Taranto-Montemurro L, Wellman A, Carberry JC, Eckert DJ. Different antimuscarinics when combined with atomoxetine have differential effects on obstructive sleep apnea severity. J Appl Physiol (1985). 2021 May 1; 130(5):1373-1382. doi: 10.1152/japplphysiol.01074.2020. Epub 2021 Mar 18 PMID: 33734828; PMCID: PMC8424567. – https://pubmed.ncbi.nlm.nih.gov/33734828/
(7) Niakani S, Liu H, Liu WY, Horner RL. Differential pharmacological and sex-specific effects of antimuscarinic agents at the hypoglossal motor nucleus in vivo in rats. Sci Rep. 2022 Sep 1; 12(1):14896. doi: 10.1038/s41598-022-19233-1. PMID: 36050440; PMCID: PMC9437041. – https://pubmed.ncbi.nlm.nih.gov/36050440/
(8) Thomson LDJ, Landry SA, Joosten SA, Mann DL, Wong AM, Cheung T, Adam M, Beatty CJ, Hamilton GS, Edwards BA. A single dose of noradrenergic/serotonergic reuptake inhibitors combined with an antimuscarinic does not improve obstructive sleep apnea severity. Physiol Rep. 2022 Aug; 10(16):E15440. doi: 10.14814/phy2.15440. PMID: 36029192; PMCID: PMC9419156. – https://pubmed.ncbi.nlm.nih.gov/36029192/
(9) Altree TJ, Aishah A, Löffler KA, Grunstein RR, Eckert DJ. The norepinephrine reuptake inhibitor reboxetine alone reduces obstructive sleep apnea severity: a double blind, placebo controlled, randomized, cross-over trial. J Clin Sleep Med. 2022 Aug 25. doi: 10.5664/jcsm.10256. Epub ahead of print. PMID: 36004739 – https://pubmed.ncbi.nlm.nih.gov/36004739/
(10) Mason M, Welsh EJ, Smith I. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2013 May 31; (5):CD003002. doi: 10.1002/14651858.CD003002.pub3. PMID: 23728641. – https://pubmed.ncbi.nlm.nih.gov/23728641/
(11) Mason M, Cates CJ, Smith I. Effects of opioid, hypnotic and sedating medications on sleep-disordered breathing in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2015 Jul 14; (7):CD011090. doi: 10.1002/14651858.CD011090.pub2. PMID: 26171909 – https://pubmed.ncbi.nlm.nih.gov/26171909/
Sleep apnea syndrome – pregnancy
Obstructive sleep apnea remains underdiagnosed in pregnancy and can lead to severe maternal and fetal complications. The risk group includes women with an elevated body mass index (BMI), older age and chronic high blood pressure. (1)
Sources
(1) Tayade S, Toshniwal S. Obstructive Sleep Apnea in Pregnancy: A Narrative Review. Cureus. 2022 Oct 17; 14(10):E30387. doi: 10.7759/cureus.30387. PMID: 36407139; PMCID: PMC9668203. – https://pubmed.ncbi.nlm.nih.gov/36407139/
Sleep apnea syndrome – overactive sympathetic nervous system
It has been proven that SAS patients have increased sympathetic nervous system activity at night and even when awake compared to healthy or overweight people without SAS. The extreme peak values that can be observed during apnea phases (up to +200%) are striking. (1) Interestingly, no correlations could be shown between the increased sympathetic nervous system activity and body mass index, AHI and blood pressure. Thus, the increased sympathetic nervous system activity may be a symptom of the stress that respiratory arrests convey to the body.
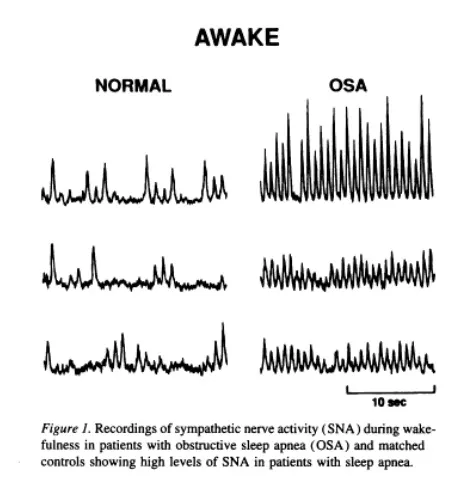
Activity of the sympathetic nervous system in people without and with SAS while awake
Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC185826/?page=2
Sources
(1) Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995 Oct; 96(4):1897-904. doi: 10.1172/JCI118235. PMID: 7560081; PMCID: PMC185826. – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC185826/?page=2
Sleep apnea syndrome - a systemic disease?
Although the strong link between SAS and obesity and other conditions was recognized early on, medicine has long treated sleep apnea as a "local abnormality" of the airways rather than a systemic disease. (1) As more and more "side effects" and connections of sleep apnea have been uncovered to date, it is clear that there is more to it than just being overweight. Significant factors are unprocessed stress and anxiety.
Sources
(1) Vgontzas AN, Bixler EO, Chrousos GP. Sleep apnea is a manifestation of the metabolic syndrome. Sleep Med Rev. 2005 Jun; 9(3):211-24. doi: 10.1016/j.smrv.2005.01.006. PMID: 15893251. – https://pubmed.ncbi.nlm.nih.gov/15893251/
Sleep apnea syndrome - Causes
The most common direct cause is narrowing of the airways due to excessive relaxation of the muscles around the upper airways during sleep.
So far, two factors have been identified that occur conspicuously often together with sleep apnea syndrome: high body weight and snoring. In habitual snorers, the moderate and severe forms of sleep apnea syndrome are more common. Overweight or obesity, especially a larger neck circumference, significantly increase the likelihood of respiratory arrest. If both factors – obesity and snoring – are present, the incidence of SAS increases even more, even in children. (1)(2) Researchers see the spreading obesity epidemic as a significant circumstance for the noticeable increase in sleep-disordered breathing in the last 30 years.
Metabolic syndrome increases the likelihood of sleep apnea regardless of the factors already mentioned. (2)(3)(4) In the presence of metabolic syndrome, the proportion of SAS in a study group can increase to 60% or more. (5) Conversely, SAS exacerbates the risks associated with obesity and metabolic syndrome.
Smoking: The data on smoking as a cause is ambiguous. It has been proven that smoking worsens the quality of sleep. Whether SAS is also a consequence remains open at the moment – there are studies that speak for and those that speak against it. (6) Pataka et al. found a reduced AHI when using a nicotine inhibitor, but the quality of sleep was worse. (7) Another study suggested that smoking could be an exacerbating factor in the presence of obesity. (8)
Read more about "Sleep apnea syndrome – menopause"
Sources
(1) Pin Arboledas G, Roselló AL, Alarcó MC, Safort MM. Epidemiología. Factores de riesgo y factores genéticos [Epidemiology. Risk factors and genetic influence]. Acta Otorrinolaringol Esp. 2010 Dec; 61 Suppl 1:7-13. doi: 10.1016/S0001-6519(10)71239-5 https://pubmed.ncbi.nlm.nih.gov/21354487/ 21354487.
(2) Verhulst SL, Van Gaal L, De Backer W, Desager K. The prevalence, anatomical correlates and treatment of sleep-disordered breathing in obese children and adolescents. Sleep Med Rev. 2008 Oct; 12(5):339-46. doi: 10.1016/j.smrv.2007.11.002. Epub 2008 Apr 11. PMID: 18406637. – https://pubmed.ncbi.nlm.nih.gov/18406637/
(3) Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, Mooser V, Preisig M, Malhotra A, Waeber G, Vollenweider P, Tafti M, Haba-Rubio J. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015 Apr; 3(4):310-8. doi: 10.1016/S2213-2600(15)00043-0. Epub 2015 Feb 12 25682233. PMCID: PMC4404207. – https://pubmed.ncbi.nlm.nih.gov/25682233/
(4) Vgontzas AN, Bixler EO, Chrousos GP. Sleep apnea is a manifestation of the metabolic syndrome. Sleep Med Rev. 2005 Jun; 9(3):211-24. doi: 10.1016/j.smrv.2005.01.006. PMID: 15893251. – https://pubmed.ncbi.nlm.nih.gov/15893251/
(5) Dräger LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstructive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. J Am Coll Cardiol. 2013 Aug 13; 62(7):569-76. doi: 10.1016/j.jacc.2013.05.045. Epub 2013 Jun 12. PMID: 23770180; PMCID: PMC4461232. – https://pubmed.ncbi.nlm.nih.gov/23770180/
(6) Pataka A, Kotoulas S, Kalamaras G, Tzinas A, Grigoriou I, Kasnaki N, Argyropoulou P. Does Smoking Affect OSA? What about Smoking Cessation? J Clin Med. 2022 Aug 31; 11(17):5164. doi: 10.3390/jcm11175164. PMID: 36079094; PMCID: PMC9457519. – https://pubmed.ncbi.nlm.nih.gov/36079094/
(7) Pataka A, Frantzidis C, Kalamaras G, Gkivogkli P, Kotoulas S, Nday C, Chriskos P, Karagianni M, Styliadis C, Paraskevopoulos E, Kourtidou-Papadeli C, Bamidis P. Varenicline administration for smoking cessation may reduce apnea hypopnea index in sleep apnea patients. Sleep Med. 2021 Dec;88:87-89. doi: 10.1016/j.sleep.2021.10.002. Epub 2021 Oct 13 PMID: 34740170 – https://pubmed.ncbi.nlm.nih.gov/34740170/
(8) Esen AD, Akpinar M. Relevance of obstructive sleep apnea and smoking: Obstructive sleep apnea and smoking. Fam Pract. 2021 Mar 29; 38(2):181-186. doi: 10.1093/fampra/cmaa112. PMID: 33128376 – https://pubmed.ncbi.nlm.nih.gov/33128376/
Sleep apnea syndrome - overweight
Obstructive sleep apnea causes or intensifies obesity. It is thought that obese individuals have large deposits of fat in their necks, which cause the upper airways to collapse in the supine position during sleep. In addition, it has been medically proven that the body can only burn fat or break down stored fat deposits during a restful sleep. So, a vicious circle. As a result, it is extremely difficult for overweight sleep apnea sufferers to fight the excess pounds. (1)
Since obesity is a significant risk factor for sleep apnea syndrome, several studies have already been carried out on how well a lifestyle change with the aim of weight loss affects sleep apnea. Both an adjustment of diet and more exercise led to a very significant reduction in AHI and thus sleep apnea via weight loss. (2)
A meta-analysis from 2006 showed that weight loss in obese people (mean baseline BMI = 46.8 kg/m2; range = 32.30-68.80) significantly improved their health profile. Diabetes was eliminated in 76.8% of patients, hypertension in 61.7%, hyperlipidemia in 70% and SAS in 85.7% of patients. This shows that obesity is a very important factor in SAS, diabetes and high blood pressure, and that SAS is highly unlikely to cause diabetes and hypertension independently. (1)
Sources
(1) Medical Advisory Secretariat. Polysomnography in patients with obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser. 2006; 6(13):1-38. Epub 2006 Jun 1. PMID: 23074483; PMCID: PMC3379160. – https://pubmed.ncbi.nlm.nih.gov/23074483/
(2) Ghitea TC, Aleya L, Tit DM, Behl T, Stoicescu M, Sava C, Iovan C, El-Kharoubi A, Uivarosan D, Pallag A, Bungau S. Influence of diet and sport on the risk of sleep apnea in patients with metabolic syndrome associated with hypothyroidism – a 4-year survey. Environ Sci Pollut Res Int. 2022 Apr; 29(16):23158-23168. doi: 10.1007/s11356-021-17589-x. Epub 2021 Nov 20 PMID: 34802081 – https://pubmed.ncbi.nlm.nih.gov/34802081/
Sleep apnea syndrome - menopause
With increasing age, especially after menopause, the proportion of women who snore grows and with it the number of women with sleep apnea. The reason for this seems to be largely the hormonal change at the beginning of menopause. During menopause, estrogen, progesterone and serotonin levels decrease and sleep disorders increase. (1) This gradually leads to a sagging of tissue, including in the mouth/throat. (2) Interestingly, hormone replacement therapy is associated with a significantly reduced risk of SAS. (3)
Sources
(1) Tandon VR, Sharma S, Mahajan A, Mahajan A, Tandon A. Menopause and Sleep Disorders. J Midlife Health. 2022 Jan-Mar; 13(1):26-33. doi: 10.4103/jmh.jmh_18_22. Epub 2022 May 2 35707298. PMCID: PMC9190958. – https://pubmed.ncbi.nlm.nih.gov/35707298/
(2) Sigurðardóttir ES, Gislason T, Benediktsdottir B, Hustad S, Dadvand P, Demoly P, Franklin KA, Heinrich J, Holm M, van der Plaat DA, Jõgi R, Leynaert B, Lindberg E, Martinez-Moratalla J, Sainz De Aja L, Pesce G, Pin I, Raherison C, Pereira-Vega A, Real FG, Triebner K. Female sex hormones and symptoms of obstructive sleep apnea in European women of a population-based cohort. PLoS One. 2022 Jun 22; 17(6):E0269569. doi: 10.1371/journal.pone.0269569. PMID: 35731786; PMCID: PMC9216532. – https://pubmed.ncbi.nlm.nih.gov/35731786/
(3) Azman M, Sani A, Kamaruddin NA. Insulin resistance using HOMA model in obstructive sleep apnea: a cross sectional study. Ann Saudi Med. 2014 Nov-Dec; 34(6):476-81. doi: 10.5144/0256-4947.2014.476 25971819. PMCID: PMC6074568. – https://pubmed.ncbi.nlm.nih.gov/25971819/
Sleep apnea syndrome - significance in science
If we look at the number of scientific research papers, the importance of sleep apnea syndrome (SAS) for everyday medical practice has increased very significantly. Currently (December 2022) there are more than 50,000 results on Pubmed Central with the keyword "Obstructive Sleep Apnea". The vast majority dates from the period after 2010. (1)
Sources
(1) Pubmed Central – https://www.ncbi.nlm.nih.gov/search/all/?term=Obstructive%20Sleep%20Apnea
Sleep Laboratory
A sleep lab is an element in diagnosing sleep apnea. If symptoms suggest sleep apnea, this is clarified in a sleep laboratory or with a mobile device at home (somnological diagnosis). Here, the person's behavior during sleep is recorded, the number of respiratory arrests and the drop in oxygen levels in the blood are measured.
Snoring
Snoring (rhonchopathy) is surprisingly widespread. About 60% of men and 40% of women snore. There is an anatomical reason why men snore more often – they naturally have narrower airways than women. The fact that children also snore should not be overlooked or dismissed. The consequences are the same as for adults: reduced regeneration, daytime sleepiness and lack of concentration. (1)(2)(3)(4)
In addition, there are many other causes why a person snores: polyps, tonsillitis, enlarged palatine or pharyngeal tonsils, reduced muscle tone in the throat and tongue, long soft palate or uvula, sinus infections, narrowed airways, cold/nasal congestion, obesity, alcohol before bed.
Most of these causes can be clarified with the help of a doctor. As a rule, snoring is harmless to health. It becomes dangerous when the quality of sleep suffers or the oxygen supply is impaired. (5)
A change in lifestyle often makes very good improvements, e.g.
- not sleeping on your back, but on your side
- raise the head of the bed
- use more than one pillow
- Refrain from sleeping pills
- drinking little or no alcohol before going to bed
- Reduce body weight
- healthy diet
- breathing through the nose / practicing nasal breathing
- Gluing the mouth shut
If this does not lead to a significant reduction in snoring, the option is to use a snoring splint (protrusion splint). The best results are achieved in snorers with the so-called tongue base snoring.
Sources
(1) Shetty M, Perera A, Kadar M, Tan B, Davey MJ, Nixon GM, Walter LM, Horne RS. The effects of sleep disordered breathing on sleep spindle activity in children and the relationship with sleep, behavior and neurocognition. Sleep Med. 2022 Dec 1;101:468-477. doi: 10.1016/j.sleep.2022.11.028. Epub ahead of print. PMID: 36521367 – https://pubmed.ncbi.nlm.nih.gov/36521367/
(2) Electroencephalography – https://de.wikipedia.org/wiki/Elektroenzephalografie#Schlafspindeln
(3) McGlinchey EL, Rigos P, Kim JS, Muñoz Nogales J, Valentine M, Kim J, Ripple CH, Wolfson AR, Alfano CA. Foster Caregivers' Perceptions of Children's Sleep Patterns, Problems, and Environments. J Pediatr Psychol. 2022 Nov 28:jsac087. doi: 10.1093/jpepsy/jsac087. Epub ahead of print. PMID: 36440553 – https://pubmed.ncbi.nlm.nih.gov/36440553/
(4) Benbir Senel G, Aktan Suzgun M, Bibinoglu Amirov C, Karadeniz D. The Comparison of the Sleep Structure and Sleep Spindle Activity in Children With Primary Snoring and Sleep-Disordered Breathing. Clin Pediatr (Phila). 2022 Nov 25:99228221139985. doi: 10.1177/00099228221139985. Epub ahead of print. PMID: 36433642. – https://pubmed.ncbi.nlm.nih.gov/36433642/
(5) Snoring splint – https://www.ergo.de/de/Ratgeber/zahngesundheit/zahnkorrektur-erwachsene/schnarchschiene
Snoring splint (protrusion splint)
The oral aids used in SAS can be divided into two broad categories: mandibular advancement splints, also known as mandibular repositioning devices or protrusion splints, and tongue repositioning or holding devices.
The user only wears a protrusion splint or snoring splint when sleeping. The wearing comfort is similar to that of braces or a grinding splint. It causes the lower jaw and tongue to be gently pushed forward. This change makes it easier to inhale and exhale and ensures that the body receives sufficient oxygen.
Snoring splints are available in the form of monobloc or bibloc splints. Monobloc splints consist of one piece for the lower and upper jaw. This makes them very quick to produce. With well-fitting protrusion splints, the success rate is high: 80 to 90% of users manage to stop snoring.
Biblock splints, on the other hand, consist of two sections, each for a jaw. These are connected to each other by flexible joints or rubber bands. The great advantage of the Biblock rail is its flexibility. However, it takes some getting used to at first, especially if the entire advance path of the lower jaw is done at once. This often causes symptoms in the first few weeks.
Types of protrusion splints: a) simple splints
Simple snoring splints are usually made of plastics of different hardness and are not individually adapted to the patient's jaw. They represent the very quick solution. These inexpensive ready-made models usually have standard sizes and can only be adjusted a little. So-called "boil and bite" splints are thermoplastically deformable and can be fitted at home. They are made of a material that is softened in a hot water bath and can then be shaped by a denture impression. Although this fine-tuning is lacking in jaws, they have one advantage: they are directly applicable. However, they are out of the question as a permanent solution because they do not fit exactly and are not durable. Costs: 20 to 50 euros for ready-made models and about 150 euros for "boil and bite" rails
There are also models that are made in the way described above, but are then reworked by the dentist.

Model of a simple plastic rail
Source: Life (Basel). 2022 Jun; 12(6): 835th Publ. online 2022 Jun 2 doi: 10.3390/life12060835
Types of protrusion splints: b) Splint created by the dentist
The highest wearing comfort is offered by splints created from an impression of the dentition. Like dental prostheses, these have an exact fit. Using the impression, the splint is then manufactured in the dental technology laboratory. At this point, there is a choice between a plastic splint and a robust, lightweight metal splint, such as the AirwayPerfect.
-> Learn more about AirwayPerfect on the patient page
These splints have the advantage, among others, that they can be used by denture wearers and that they can also be fitted to individuals with tooth gaps. Even if tooth loss occurs during the wearing period, the AirwayPerfect can be easily adjusted. The costs for a medical splint range between €1000 and €1800. If prescribed by a general practitioner or sleep specialist, the health insurance company covers a portion of the costs.

AirwayPerfect optimally adapted to the user's dentition
(click on the image for a full view)
Protrusion Splint - Durability
The lifespan of protrusion splints is influenced by their use and dental care. This is because the plastic material is fundamentally deformable, which can easily lead to damage and breakage. The AirwayPerfect is therefore made of steel and thus has an almost unlimited lifespan.
Protrusion splint - possible side effect
Muscle pain and tension in the jaw, foreign body sensation, dry mouth, cough, increased salivation, tooth and gum pain (1)
Sources
(1) Mohammadieh AM, Sutherland K, Chan ASL, Cistulli PA. Mandibular Advancement Splint Therapy. Adv Exp Med Biol. 2022;1384:373-385. doi: 10.1007/978-3-031-06413-5_22 https://pubmed.ncbi.nlm.nih.gov/36217096/ 36217096.
Protrusion Splint - Cleaning
It is best to clean splints – no matter which ones – just as well as braces or dentures. Cleaning after each application is ideal.
Protrusion splint - comparative studies
A Dutch study from 2022 compared the benefits of an individually precisely fitted protrusion splint (SPS) compared to a protrusion splint (SPS) produced in a rapid process. The study ran over two 12-week periods and showed – objectively and subjectively determined – that both types of a protrusion splint produced the same improvement. What was unfavorable about the study was the low average initial AHI of 16.3. The 12-week duration is also too short to test the tolerance and motivation of those affected to wear a splint in the long term. However, the researchers come to a helpful conclusion: A PLC can be used to test the benefits of this tool before an adapted protrusion splint is made. (1)
Sources
(1) Bosschieter PFN, Uniken Venema JAM, Vonk PE, Ravesloot MJL, Hoekema A, Plooij JM, Lobbezoo F, de Vries N. Equal effect of a noncustom vs a custom mandibular advancement device in treatment of obstructive sleep apnea. J Clin Sleep Med. 2022 Sep 1; 18(9):2155-2165. doi: 10.5664/jcsm.10058. PMID: 35532113; PMCID: PMC9435323. – https://pubmed.ncbi.nlm.nih.gov/35532113/
One study compared CPAP and protrusion splint in terms of effects on cardiovascular factors after one year. Neither agent achieved any improvements except for the AHI value. (1) This was confirmed by another study that ran for a year. Subjects who were assigned to a group stayed in it for the whole year without changing methods. In contrast to the previous study, the oxygen level in the blood was better in the CPAP group. There were no changes in blood pressure in either group. However, the tolerance to wear the mask was much worse than with the splint. 42% could not get used to wearing the mask permanently, compared to only 16% who used the protrusion splint irregularly at night. (2) This tendency to wear the splint for longer compared to CPAP was also shown in two other studies. In the first, the AHI dropped significantly after one month to 11 (splint) and 4.5 (CPAP). The splint showed advantages in quality of life compared to CPAP, while blood pressure did not improve with either method. (3) In the second study over 4 to 6 weeks, 4.6% of the participants found neither CPAP nor protrusion splint to be an acceptable solution. Similar results as before: slight benefits in quality of life for the splint and only very slight changes in arterial blood pressure (2.5 and 2.2 mmHg, respectively) in patients with hypertension. (4)
Sources
(1) Uniken Venema JAM, Knol-de Vries GE, van Goor H, Westra J, Hoekema A, Wijkstra PJ. Cardiovascular and metabolic effects of a mandibular advancement device and continuous positive airway pressure in moderate obstructive sleep apnea: a randomized controlled trial. J Clin Sleep Med. 2022 Jun 1; 18(6):1547-1555. doi: 10.5664/jcsm.9908. PMID: 35088708; PMCID: PMC9163609. – https://pubmed.ncbi.nlm.nih.gov/35088708/
(2) Guimarães TM, Poyares D, Oliveira e Silva L, Luz G, Coelho G, Dal Fabbro C, Tufik S, Bittencourt L. The treatment of mild OSA with CPAP or mandibular advancement device and the effect on blood pressure and endothelial function after one year of treatment. J Clin Sleep Med. 2021 Feb 1; 17(2):149-158. doi: 10.5664/jcsm.8822. PMID: 32964829; PMCID: PMC7853217. – https://pubmed.ncbi.nlm.nih.gov/32964829/
(3) Phillips CL, Grünstein RR, Darendeliler MA, Mihailidou AS, Srinivasan VK, Yee BJ, Marks GB, Cistulli PA. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013 Apr 15; 187(8):879-87. doi: 10.1164/rccm.201212-2223OC. PMID: 23413266. – https://pubmed.ncbi.nlm.nih.gov/23413266/
(4) White DP, Shafazand S. Mandibular advancement device vs. CPAP in the treatment of obstructive sleep apnea: are they equally effective in Short term health outcomes? J Clin Sleep Med. 2013 Sep 15; 9(9):971-2. doi: 10.5664/jcsm.3008. PMID: 23997711; PMCID: PMC3746726. – https://pubmed.ncbi.nlm.nih.gov/23997711/
Provided that users use their CPAP device or their protrusion splint in the long term, good results can be achieved with both. One study compared exactly this in a 10-year follow-up. The approximately 30% who persevered had both achieved an average AHI of less than 10 and were therefore no longer sleep apnea patients. The data show that almost all of them had reached this low value after just one year and were able to maintain it through the continued use of splint or CPAP. (1)
Sources
(1) Uniken Venema JAM, Doff MHJ, Joffe-Sokolova D, Wijkstra PJ, van der Hoeven JH, Stegenga B, Hoekema A. Long-term obstructive sleep apnea therapy: a 10-year follow-up of mandibular advancement device and continuous positive airway pressure. J Clin Sleep Med. 2020 Mar 15; 16(3):353-359. doi: 10.5664/jcsm.8204. Epub 2020 Jan 14. PMID: 31992403; PMCID: PMC7075089. – https://pubmed.ncbi.nlm.nih.gov/31992403/
Protrusion splint - Advantages
Protrusion splint therapy is the best alternative to CPAP therapy in the treatment of obstructive sleep apnea. There is still a high percentage of patients who need an alternative for CPAP due to intolerance, inconsistent use (poor compliance) or subjective rejection. The situation is similar with the various surgical treatments. Here, many find it difficult to muster the necessary high motivation for this permanent change in the throat. (1)(2)
According to studies, the protrusion splint is no better than CPAP in lowering the apnea-hypopnea index (AHI). However, it has been shown to be equivalent to CPAP in a number of important neurobehavioral and cardiovascular health outcomes. This means that the simpler solution of a splint is clearly advantageous for the patient due to the lower effort and the smaller changeover. The health effect on the comorbidities may be due to the better tolerability and higher treatment adherence of the patients compared to CPAP. (3)
Sources
(1) ENT guidebook: Sleep apnea syndrome: Alternatives to the mask – https://www.youtube.com/watch?v=qXYLKTpbeQA
(2) Verbraecken J, Dieltjens M, Op de Beeck S, Vroegop A, Braem M, Vanderveken O, Randerath W. Non-CPAP therapy for obstructive sleep apnoea. Breathe (Sheff). 2022 Sep; 18(3):220164. doi: 10.1183/20734735.0164-2022. Epub 2022 Oct 11 36340820. PMCID: PMC9584565. – https://pubmed.ncbi.nlm.nih.gov/36340820/
(3) Mohammadieh AM, Sutherland K, Chan ASL, Cistulli PA. Mandibular Advancement Splint Therapy. Adv Exp Med Biol. 2022;1384:373-385. doi: 10.1007/978-3-031-06413-5_22 https://pubmed.ncbi.nlm.nih.gov/36217096/ 36217096.
Protrusion splint - effect
What exactly a protrusion splint does is still unclear, because several changes have been observed, depending on the anatomy of the throat. (1) Undoubtedly, the splint leads to a repositioning of the lower jaw and thus contributes to a greater opening of the upper airways as well as reduced collapse of the airways at night.
The researchers of the study "Pharyngeal Airspace Alterations after Using the Mandibular Advancement Device in the Treatment of Obstructive Sleep Apnea Syndrome" (Ferraz et al., 2022) want to sensitize doctors to the need to examine the oral cavity. This is because it can be increasingly involved in the pathophysiology of SAS, so that the examination can make a valuable contribution to screening. (1)
Cephalometric lateral image without protrusion splint (A) and one year after treatment with protrusion splint inserted (B).
Source: Life (Basel). 2022 Jun; 12(6): 835. Published online 2022 Jun 2. doi: 10.3390/life12060835
(please click on image for full view)
Sources
(1) Ferraz PD, Francisco I, Borges MI, Guimarães A, Carvalho F, Caramelo F, Figueiredo JP, Vale F. Pharyngeal Airspace Alterations after Using the Mandibular Advancement Device in the Treatment of Obstructive Sleep Apnea Syndrome. Life (Basel). 2022 Jun 2; 12(6):835. doi: 10.3390/life12060835. PMID: 35743866; PMCID: PMC9224702. – https://pubmed.ncbi.nlm.nih.gov/35743866/
How do your patients get the AirwayPerfect splint?

It's very easy: We take care of the entire coordination for you!
We, Büchner Zahntechnik, handle the entire process, including appointment scheduling at the sleep lab, contact with the statutory health insurance company regarding cost coverage, cooperation with the dentist, and the production of your AirwayPerfect. You advise your patient and take an impression – we take care of everything else.
Even if the patient has problems with the AirwayPerfect, we are the first point of contact. We intervene promptly to find a solution that allows the patient to continue using the splint comfortably.
Sounds good? Then we should make a personal appointment. I will demonstrate an original splint to you and we will discuss all the details from A to Z, from anamnesis to co-payment.
Call me (Tel. 06204-961730) or send me a message via the contact form. I will get back to you immediately.
Yours,
Meinhard Büchner
